Epilepsy is a common neurological condition in which patients suffer recurrent seizures (also referred to as convulsions).
A generalized convulsion is a rather dramatic event. If it occurs while the patient is standing, frequently the patient gets no warning and falls down striking the ground hard. This is the time injuries occur. As the patient is falling down, he/she is amnestic for the entire episode. Family/bystanders notice that initially the patient stiffens (arms and legs are extended, eyes are rolled up into the head, clenching of the teeth occurs which at times leads to the tongue getting bitten, the patient may at times suffer loss of bladder control). This “tonic” phase is followed by the “clonic” phase during which convulsive movements occur. The seizure stops in a minute or two but the patient remains unresponsive and slowly regains consciousness.
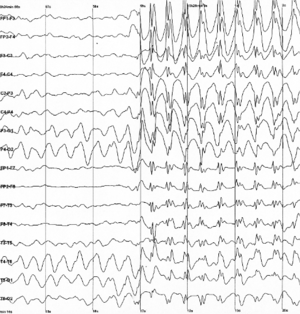
If the above convulsion occurs WHILE the patient is undergoing an EEG test (electroencephalogram), the abnormal brain activity is picked up by the test (see example below) and the diagnosis confirmed.
Based on the misfiring recorded on the EEG, the neurologist can then opine what kind of epilepsy the patient has and where (which part) in the brain the seizures are originating from.
EEG showing abnormal brain waves (spike wave discharges) and beginning of a seizure (IMAGE SOURCE: Wikipedia-the image is used for purely educational purpose)
WHEN A SEIZURE IS NOT A SEIZURE–LET US TALK ABOUT PSEUDOSEIZURES
Pseudoseizure is the term used for events that appear to be epileptic seizures but, in fact, are not. So while the patient may have a dramatic event where in he/she shakes, may roll up the eyes, arch his back, moan, make noises and vocalize, THERE IS NO ABNORMAL EXCESSIVE SYNCHRONOUS CORTICAL ACTIVITY (meaning that on the EEG, the brain waves appear normal without any misfiring).
Pseudoseizures are referred to by various names such as psychogenic non-epileptic events (PNES), non epileptic events (NEE), non epileptic seizures, hysterical seizures.
When pseudoseizures are suspected, a neurologist or epileptologist (epilepsy specialist) shall take a detailed history, may order a MRI scan of the brain and then attempt to capture one of these events on VIDEO-EEG MONITOR (Video-EEG is a special kind of EEG in which simultaneous EEG and video recording of the patient is carried out). The goal is to capture one of the patient’s reported events on video-EEG. If no misfiring of the brain is observed during the event, a diagnosis of pseudoseizures is made.
The non-epileptic (“YOU DO NOT HAVE EPILEPSY” OR “THESE ARE NOT SEIZURES”) nature of the events is then explained to the patient and the family and an attempt is made to try to determine the underlying cause (Why is the patient having these events?). There are many causes of pseudoseizures such as mental stress, sexual or physical abuse, personality disorders, dissociative disorders, affective disorders (mood disorder, anxiety, depression), substance abuse disorder, family conflict, conflict or stress at work, problems in marriage among others.
The treatment is usually a combination of psychotherapy and use of medications (selective serotonin reuptake inhibitors). With support and understanding most patients start to improve and the events either stop completely or become less frequent.
April 30th, 2010 dawned just like any other April day. As the sun rose along the eastern seaboard, Manhattan came to life with its golden rays. A healthy glow permeated all around. But not all its residents were blessed with this good health. Saint Vincent was sick, terminally sick with multi organ failure. Its corridors once bustling with doctors and nurses in scrubs lay deserted. Its emergency department once full of patients was eerily quiet. Its intensive care units once a melody of ventilator hums and telemetry monitor beeps were quiet as if a great orchestra had played its last composition. Its cafeteria once full of hungry overworked residents had served its last meal. The end had come slowly but now the writing was on the wall. Terminally ill with no hope of a meaningful recovery they said as they went by. The hospital which had once given the gift of life to so many now itself lay on its death bed. Where critically ill patients once received life-saving infusions of antibiotics found itself deserted in its final battle for survival. Saint Vincent found no one to turn to, no one to hold its hand and no one to administer CPR (cardiopulmonary resuscitation). It thought it was too big to fail but no one stepped forward to bail it out. Saint Vincent hospital died on April 30th, 2010.
Image Source: CNN (the picture is purely for information and education purpose)
Saint Vincent’s Hospital or Vinny’s as the residents affectionately referred to it was a large hospital situated in the heart of the West Village. For more than 150 years it served the residents of New York. 1 This is the hospital where the HIV epidemic first exploded in the late 80’s/ early 90s and where the battle against this disease was fought and ultimately won. Vinny was also at the forefront of providing care and comfort when New York City was attacked on September 11th, 2001. If Vinny had not been allowed to die on that fateful day in 2010, it would have certainly opened its wide arms to take care of coronavirus (COVID-19) stricken New Yorkers young and old. Precious lives would have been saved if only Vinny was alive today.
American football, soccer, rugby, ice hockey, boxing, mixed martial arts, and wrestling are popular contact and combat sports both in the United States and in countries around the world. In these sports head impact exposures resulting in concussions are common. In American football, rugby and soccer, concussive injuries to the brain occur accidently when there is contact of the player’s head with the opposing player(s) head, torso, turf or as occurs in soccer with the ball while heading. In boxing every punch thrown at the head is thrown with the intention of winning by causing a knockout. As a result, concussions, and acute traumatic brain injuries such as subdural and epidural hematoma are common. Subdural hematoma is the most common cause of boxing related mortality. In recent years, the risk of chronic traumatic encephalopathy (CTE), a chronic neurodegenerative disorder associated with contact and combat sports has garnered the attention of physicians, players, and fans.
Concussion definition and evaluation
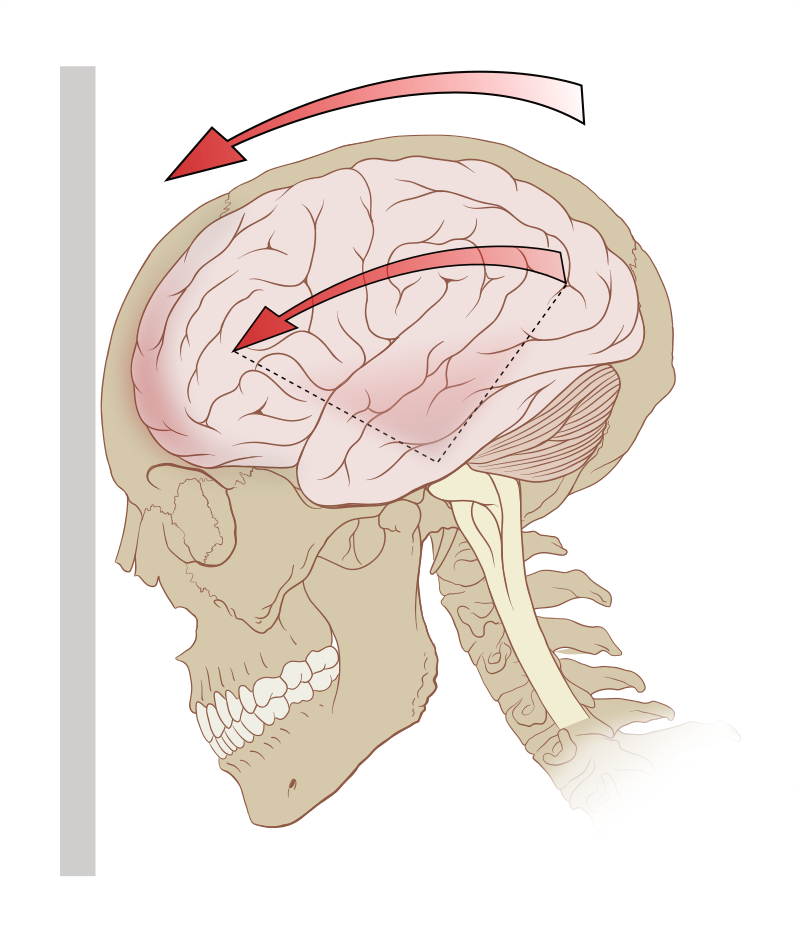
Concussion is defined as a clinical syndrome characterized by immediate and transient alteration in brain function, including alteration of mental status and level of consciousness, resulting from mechanical force or trauma. It is important to remember that loss of consciousness is not required for a concussion. Concussions are informally and non-scientifically graded into mild, moderate, and severe based on the duration of loss of consciousness and post traumatic amnestic period. Concussive properties of any head impact exposure depend upon the force, velocity, and angle of the hit to the cranium and how the mechanical forces are transferred and absorbed through the intracranial cavity. Both linear and rotational (angular) acceleration forces play a role as does impact deceleration occurring when the athlete falls and strikes the head against the ground.
Image Credit: Patrick J. Lynch, medical illustrator – Modified version of Image: Skull and brain normal human.svg by Patrick J. Lynch, medical illustrator (Source Wikipedia). The image is solely for educational purposes only.
The nature of many contact and combat sports is such that head impact exposures cannot be altogether avoided. Abundant medical literature highlights the long-term health significance of multiple head impact exposures.Minor concussions (sub concussive injuries) contribute to the development of CTE, a neurodegenerative disorder presenting with a constellation of cognitive, mood, and behavioral changes along with motor system dysfunction (Parkinsonism) usually after the athlete has retired. The symptoms of concussion are predominantly subjective such as headache, dizziness, nausea, light sensitivity, sound sensitivity, and cognitive dysfunction. Frequently, when athletes sustain head impact exposures, they themselves are unaware that they are concussed and continue to play. As a result, it is important that when an athlete sustains a head impact exposure, a standardized concussion evaluation be conducted. While this can be conducted on the sidelines, evaluation in the locker room where the athlete is less likely to be distracted is more ideal. Since some athletes exhibit motor signs such as impaired coordination, balance, and stance after a concussion while others exhibit only cognitive dysfunction, it is important that multimodal concussion evaluation be conducted. This includes use of Maddocks questions to gauge awareness, standardized concussion assessment tools such as SCAT5, King Devick test and Balance Error Scoring System (BESS).
Concussions are common in soccer especially during heading the ball.
Management of concussive injury
The athlete’s mentality is to never quit. Hence many athletes will deny symptoms of a concussive injury to the brain. Physicians should be aware of this. An athlete who has suffered a concussion should be pulled out of play and “benched.” This is done for two main reasons. A concussed athlete with impaired attention, concentration, balance, and coordination is more prone to a second head impact exposure. The other reason is that if the concussed athlete continues to play, it is likely that he or she will exhibit more profound and prolonged post-concussion symptoms. The benched athlete is advised a period of cognitive and physical rest. The rationale for this is that a concussed brain is in a state of energy crises and fares better when the cognitive and physical demands on it are less. Cognitive rest entails pulling back from cognitive activities such as team meetings, college work, screen time (amount of time spent using devices with screens such as a smartphone, computer, television, or video game console). Physical rest entails pulling back from normal physical activities such as running and jogging. Here it is important to emphasize that complete cocooning is ill-advised with recent research work showing that it may in fact be detrimental and lead to prolongation of symptoms. The concussed athlete should be evaluated by a physician skilled in concussion management. In most cases neuroimaging with computed tomography or magnetic resonance imaging is not warranted and if conducted comes back negative. There is currently no validated imaging or biofluid (blood or cerebrospinal fluid) biomarkers for concussion. In the absence of biomarkers, the diagnosis of concussion is made clinically based on history of head impact exposure followed by characteristic symptoms (post-concussion symptoms). The concussed athlete is advised to drink adequate water and to avoid alcohol intake and sudden inversions till symptomatic. The role of supplements such as magnesium, vitamin B2 (riboflavin), vitamin B12, fish oil among other remains unclear but these are frequently prescribed. There is no treatment for the head injury itself. Treatments for symptoms of concussion such as headache, dizziness, cognitive impairment, poor sleep, mood, and behavioral disorder involves a multi-disciplinary team consisting of neurologists, neuropsychologists, neurosurgeons, neuroradiologists, neuro-ophthalmologists, physical therapists, occupational therapists, and vestibular therapists with expertise in concussion management.
After a few days of cognitive and physical rest when the acute concussion symptoms have abated, the athlete begins a graded and gradual return to play (RTP) program preferably under the guidance of an athlete trainer with expertise in concussion management. Nowadays most contact and combat sports have sport specific return to play (RTP) protocols. Despite individual variations, the basis tenant remains the same and involves the athlete progressing from light aerobic activity (walking or stationary bike for 10 minutes, no resistance training) to sport-specific activity/drills to non-contact training drills to contact practice and if asymptomatic return to play after a release has been signed by the treating physician.
Conclusion
Concussion is a common head injury in contact and combat sports. Timely identification of the concussed athlete, removal from play and medical management usually results in a good outcome. Closer medical supervision of sports and education of all concerned parties on concussion recognition and management remains the need of the hour.
In this blog post, I shall discuss a number of disorders that affect the facial nerve.
The movements of the face are controlled by the facial nerve. This is the nerve which makes us smile, laugh, frown controlling numerous other facial expressions which humans possess. Facial nerve is a cranial nerve (cranial nerves, a set of 12 nerves originate in the brain). Facial nerve is cranial nerve VII (seven). The right facial nerve controls the muscles of facial expression on the right side of the face while the left facial nerve does the same for the left side of the face).
Innervation of the muscles of the face by facial nerve (cranial nerve VII) Henry Vandyke Carter and one more author – Henry Gray (1918) Anatomy of the Human Body. Image source: Facial Nerve Wikipedia. The image is on public domain and is reproduced here for educational purposes only.
There are a number of disorders which can affect the facial nerve. Some of these disorders cause twitching of the face (tics, hemifacial spasm) while others cause weakness/drooping of one side of the face (stroke, Bells palsy).
FACIALTICS
Facial tics are repeated spasms which involve different muscles of the face (such as rapid eye blinking, nose twitching, head jerking, shoulder shrugs). Tics can be classified into simple motor tics (such as those listed above) and complex motor tics (in a complex motor tic, a series of movements are performed in the same order repeatedly). While tics occur involuntary, most patients are able to stop their tics (for a short period of time) if asked to do so. “Holding the tic in” though causes distress which is relieved by performing the tic. Tics are usually considered to be harmless but they may occur multiple times during the day causing distress and become socially disabling to the patient and those around). As a result, not all tics need to be treated. If the tics are not bothering the patient per se, I usually educate the patient/family on facial tics and what can exacerbate them (stress/anxiety, lack of sleep) and keep the patient under my observation. Many children/ youth may exhibit a transient tic disorder and then grow out of it. Tourette’s Syndrome is a chronic tic disorder characterized by multiple motor and vocal tics. If tics need treatment, behavioral therapy and medications are prescribed.
HEMIFACIAL SPASMS
As the name suggests, in hemifacial spasm the patient exhibits facial muscle contractions (spasms) involving one side of the face. The disorder is characterized as a movement disorder of the facial nerve in which muscles of one side of face twitch involuntary. Hemifacial spasm occurs when something irritates the facial nerve and the cause needs investigation. The diagnosis of HS is made by a neurologist based on observing the facial movements and results of test such as MRI brain (to look and see if anything is irritating the facial nerve/its branches inside the brain).
The treatment of HS depends on the cause. Various treatment options include use of medications (anticonvulsant drugs are sometimes prescribed), botulinum toxin (BOTOX) and surgery.
In this blog post, I shall discuss various treatment options for obstructive sleep apnea (OSA). Good news is that nowadays there are a number of very effective treatment options available for OSA. Let us discuss these one by one:
Positional Sleepers: This is the simplest treatment available for snoring and at times OSA. As the name suggests, a positional sleeper helps a person sleep on his/her side as against the back. Since snoring and OSA is frequently worse on the back, sleeping on the side is helpful (the tongue falls on the side and does not obstruct the flow of air). There are many different positional sleepers available on the market. Many of my patients design their own positional sleeper by using pillows or tennis balls sewn into their T shirt/PJs.
COMMERICALLY AVAILABLE POSITIONAL SLEEPER: THIS ONE IS CALLED ZZOMA (Source: sleep education blog) no copyright infringement is intended and the image has been included for purely educational purposes.
Mandibular Advancement Device (MAD): MAD is like a mouth guard. The patient puts the MAD into his/her mouth at night before sleeping. As the name suggests the device “helps to advance the mandible/lower jaw”. The tongue is attached to the lower jaw. So the device by pulling the jaw and tongue forward helps to make more room in the back of the throat for air to flow in and out more easily. There are MADs which are available over the counter. These devices while cheaper as compared to custom made device (made by a dentist) have one problem. They usually are not well fitting. As a result they are not comfortable and are not effective. The best MAD is one which is made by a dentist. The dentist measures the patient’s teeth and makes a device which fits well, is comfortable and effective. Most dentists make MADs so please talk to your dentist about this. There are dentists who are certified by the American Academy of Dental Sleep Medicine. In my opinion these dentists are the best in MADs and I frequently refer my patients to one.
Mandibular Advancement Device (Source: myhealth.alberta.ca) no copyright infringement is intended. Image has been included for purely educational purpose.
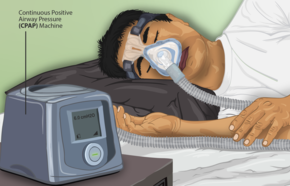
Nasal Continuous Positive Airway Pressure (CPAP): Nasal CPAP is the most effective treatment for OSA around the world. CPAP has no side effects-it is a simple machine which helps to “force” the air into the narrowed airway. The patient sleeps with a mask over the nose (nasal mask) or over the nose and mouth (full face mask). The mask is attached to the CPAP machine with the help of a long hose. In the night when the patient is about to sleep, he/she puts the mask on and turns on the machine. The machine sucks in room air, filters it (the machine can be fitted with HEPA filters), humidifies it (the machine has a small humidifier and the patient can change the setting to his/her comfort level) and then blows the air with force in to the patient’s nose. The machine does this throughout the night. In the morning when the patient gets up, the machine is turned off. Indeed a simple and effective solution to OSA. While nasal CPAP has no side-effects, there is one problem. That problem is that majority of patients initially find the CPAP uncomfortable to use. In my experience this is very common. I have patients who come back and tell me they hate the machine, they cannot sleep with the machine and that they will not use it. There are others who come back and say they love the machine and it has changed their lives. So, I tell my patients not to get dejected and upset when initially they are struggling with CPAP use. Finding the most comfortable mask, adjusting the CPAP pressure and humidifier settings wells and most patients over time begin to get used to sleeping with the machine and start to like it. The correct CPAP pressure (the pressure needed to make the OSA go away) is calculated in the Sleep Lab (patient sleeps in the Sleep Lab and while asleep the correct CPAP pressure is determined by the Sleep Medicine technician). There are numerous CPAP machines (different models made by different vendors) and many different types of masks. The trick in my opinion is to find the right mask for the patient and the correct CPAP settings. Once that is done, most patients like CPAP. I usually instruct my patients to try to use the CPAP as much as possible (goal is to get the patient to use the CPAP every night and throughout the night as many patients go to sleep with the CPAP on but then take it off during the night).
Source: CPAP. Wikipedia (no copyright infringement is intended. Image has been included for purely educational purpose).
Nitin K. Sethi, MD; Amy Wasterlain, MD candidate; Cynthia L. Harden, MD
Epilepsy is one of the most common neurological conditions. There is an enormous unmet need when it comes to the care of the epilepsy patient. A few years ago I coauthored an article on the care of pregnant women with epilepsy. I am hopeful that physicians, patients and caregivers shall find the article helpful.
When a patient with epilepsy is pregnant or planning for pregnancy, you face the challenge of balancing the benefits and teratogenic risks of her antiseizure medication. Here’s help.
It all began with my friend Nagi inviting me to be chief guest at his daughter’s Arangetram. Arangetram, the debut on-stage performance of a Bharatanatyam student after successful completion of years of arduous training under her guru is certainly a matter of immense pride and joy not only for the student but also family and friends. Ekanta had worked hard for many years to achieve this milestone and finally was about to graduate. Touched by Nagi’s affection, I readily accepted to preside over the function.
But being the chief guest meant that I would have to give a short speech to the assembled august gathering. As a neurologist I knew precious little about Bharatanatyam, the oldest classical dance tradition in India. Well maybe you can talk about the neurology of Bharatanatyam advised my son Nitin, himself a neurologist. While I had seen Bharatanatyam performances a few times, I had never studied the art form from a neurologist’s viewpoint. I opened Bradley’s Neurology in Clinical Practice and to my dismay found nothing about the neurology of dancing let alone the neurology of Bharatanatyam. After a PubMed search was unhelpful, an Internet search via Google yielded two interesting articles, one from Scientific American magazine and the other in the Journal of Aesthetic Education.
Bharatanatyam is a classical dance form from South India dating back to 1000 B.C. It is based on ‘Adavu’ (steps) and ‘Hasthamudra’ (hand gestures). The dancer expresses herself via ‘bhavabhinaya’ (facial expression) and ‘hasthamudra’. The dancer is dressed bright colors and adorned with a garland in her hair and foot trinklets. The music is Carnatic classical music yielded by instruments such as violin, flute, mridangam (South Indian drum) and veena (string plucked instrument). The nattuvanar is the most important member of the Bharatanatyam orchestra and plays a set of cymbals known as talam and sings ‘Vaaythari’ (chanting). In a Bharatnatyam performance the dancer attempts to become the character she portrays be it Rama, Krishna or his beloved Radha and mimics all actions of the Supreme as best as she can. During the duration of the program all participants, the artist and the audience alike are elevated to a spiritual dimension which the Upanishads call ‘Raso vai sah Rasam hyevayam labdhvanandi bhavati’ (he the highest self is bliss in itself). Every recital starts by invoking the blessing of Ganesha and Nataraja (the cosmic dancer) and it ends by seeking their blessings again.
The complexity of the central nervous system is evident even in the simplest of hand movements such as movement of the right index finger. Neurons in the contralateral motor strip are activated as are neurons innervating the corresponding antagonist muscles which need to relax so that movement can take place. Neural impulses travel down from the cortex via the internal capsule, mid brain, brain stem, pyramidal track, cervical spinal cord, peripheral nerve finally reaching their target muscles. The accompanying facial expressions add yet another dimension and convey a story to the spectator.
Let us take the example of ‘Shabdam’ bharatanatyam performance – a scene from the epic Mahabharata where Draupadi is in great peril. The Pandavas have just lost her to the Kauravas in a game of dice and Draupadi is forcibly brought to the court being dragged by her hair. The evil Duryodhana attempts to disrobe her by pulling her sari. The bharatanatyam artist performs this scene with just her facial expressions. A look of contempt towards her five husbands who wagered her in a game of dice and the next instant pleading with her eyes to Lord Krishna to help protect her modesty which he does so by extending the length of her sari repeatedly. At the same time the artist covers her bosom with her hands to save her modesty, eyes turned down exhibiting shame. Thus, a story involving many characters is conveyed by a single artist all with the use of hand and face gestures as well as eye movements. The artist during this complex performance is keeping time and synchronizing her actions to the vocalist who is singing and narrating the complex story. She also needs to keep pace with the music with her feet to the beat of mirdamgam.
It is indeed fascinating how the artist’s brain is able to accomplish all these complex actions simultaneously, eyes moving in different directions at times independent of each other with facial expressions changing depending on the scene as narrated by the vocalist.
Behind every bharatanatyam recital there is intense ‘tapasya’ (practice) of several hundreds of hours and repetitive rehearsals starting from a very tender age under the watchful eyes of the guru. This extra ordinary coordination of movements of the hands, eyes and facial expressions synchronized to music is indeed a testament to the wonder of the human brain and incorporates several neuronal pathways.
To hop on one foot patting your head at the same time requires calculations relating to spatial awareness, balance, intention and timing, among other things, in the brain’s sensorimotor system. A region called the posterior parietal cortex (toward the back of the brain) translates visual information into motor commands, sending signals forward to motion-planning areas in the premotor cortex and supplementary motor area. Several neuronal networks are involved. The cortical center (s) and networks perceive the sound of vocalist, sound of mridangam and taalam, coordinate and then perform appropriate hand movements, eye movements and facial expressions. Simultaneously the brain coordinates the act of dancing keep rhythm with vocalist and other musical instruments. The whole performance requires multiple neuronal circuits of brain to plan and execute. How much role do the frontal cortex, hippocampus and cerebellum part we do not know.
At present we don’t have knowledge of the whole neuronal network involvement involved to perform this complex dance form. Unlike singing where functional MRI imaging has added to our knowledge, there are no functioning MRI imaging studies for dancing. One thing which is definite is that this art can be learnt when one is young because there is lot of plasticity of brain. Dance is indeed the essence of life. Now the role of dance as a form of therapy in diseases such as Parkinson’s disease is also well established.
The Nobel laureate Eccles in his famous book “THE UNDERSTANDING OF THE BRAIN” wrote “how can a brain understand a brain”. The human brain still remains the LAST FRONTIER to conquer.
Many people snore. Do all snorers (people who snore) also suffer from sleep apnea? Is snoring harmful to health? Is sleep apnea harmful to health? What are the signs and symptoms of someone who has sleep apnea? How is sleep apnea diagnosed and treated? These and other questions shall be discussed in this blog post and the one that follows.
SNORING: simply defined snoring is noisy breathing which occurs when a person is sleeping. It is a very common condition. Many people snore when they fall asleep on their backs (supine position). Some snore softly, others snore loudly disturbing the sleep of their bed partner. Hence snoring can be of mild, moderate and severe intensity. A common cause of snoring is obstruction to the flow of air in the nose. Deviated nasal septum with or without turbinate hypertrophy is a common cause of snoring. Snoring at times can also occur when there is obstruction to airflow in the upper part of the throat. In these cases, the soft palate vibrates giving rise to the snoring sound. When snoring occurs on its own it is referred to as simple snoring.
Simple snoring is not considered to be harmful to the health of the snorer. Hence simple snoring does not need to be treated in all cases. Simple snoring though disturbs the sleep of the bed partner. It may be so loud that the bedpartner is forced to sleep in a separate room! At times patients snore so loudly that their snoring wakes them up! In these cases snoring may warrant treatment.
TREATMENT FOR SIMPLE SNORING: There are many treatment options for simple snoring. These include simple interventions such as weight loss (we are more likely to snore as we put on weight so weight loss frequently alleviates snoring), sleeping on the side (lateral position) rather than on the back (supine position) also helps. Snoring occurs most commonly when one sleeps on his/her back. Sleeping on the side with the head elevated may at times alleviate snoring completely. This can be accomplished by a number of ways. Use of POSITIONAL SLEEPERS is recommended in these patients. There are a number of positional sleepers available on the market. Many of these are over the counter and do not require a doctor’s prescription. These BUMPER BELTS all attempt to treat snoring by “forcing” the snorer to sleep on his/her side than on the back. One can also make one’s own positional sleeper with the help of pillows or a ball tied around the upper back. There are surgical treatments for simple snoring. A commonly performed surgery (done by ENT surgeons) is SEPTOPLASTY AND TURBINATE REDUCTION SURGERY. In this surgery the ENT surgeon corrects the deviated nasal septum and reduces the size of the enlarged nasal turbinates.
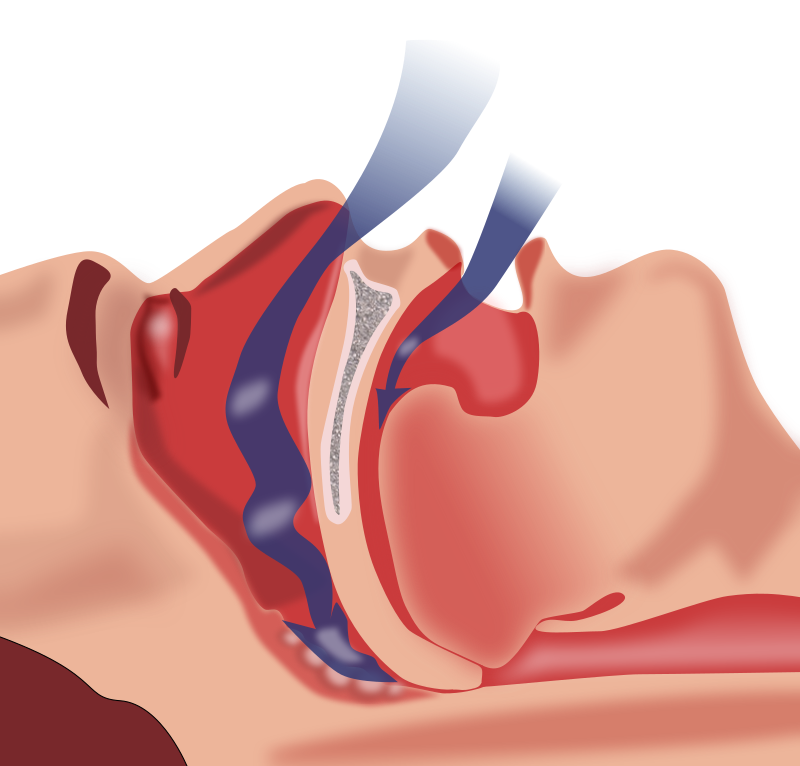
SNORING ALONG WITH SLEEP APNEA: When someone stops breathing while asleep it is referred to as sleep apnea (SA). Sleep apnea can either be obstructive (referred to as obstructive sleep apnea or OSA) or central (referred to as central sleep apnea or CSA). OSA is far more common than CSA and as the name suggests it is due to OBSTRUCTION to airflow. The obstruction occurs due to narrowing of the airway at the level of the oro-pharynx. Behind the tongue lies the airway. It is hollow tube which goes down, becomes the trachea and takes air to the lungs. In people who are overweight, the upper part of this airways gets obstructed by the tongue, “excess” soft tissue and enlarged tonsils. When these overweight people lie down on their back to sleep, the tongue falls back narrowing and obstructing airflow through the upper airway. The excess soft tissue around the neck also contributes to upper airway narrowing. The airway then collapses leading to OSA. It is important to remember that people who have OSA frequently have no complaints. They are NOT bothered by their snoring or by the episodes of sleep apnea. Their complaint (if any) is that the next day they wake feeling tired (not rested). These people feel sleepy during the day (this is referred to as EXCESSIVE DAYTIME SLEEPINESS) and may fall asleep (or struggle to stay awake) during meetings and while in class.
Many people thus do not realize they suffer from sleep apnea. They only seek medical attention when their bedpartner is bothered by their snoring or complains about their excessive daytime sleepiness.
As compared to snoring, OSA is harmful to the patient’s health. Nowadays OSA is considered to be a risk factor for hypertension (elevated blood pressure), diabetes (elevated blood sugar) and there are studies that indicate that untreated OSA increases the risk for heart disease and strokes.
While OSA is common in people who are over weight, have a thick (increased fat and soft tissue) neck and enlarged tonsils/adenoids, it can also occur in people who have normal weight and body mass index (BMI). In these people the cause of OSA is different (anatomically they may be predisposed to OSA due to the structure of their face/jaw and upper airway which predisposes to airway collapse while asleep).
In this blog post let us dwell on the management of Parkinson’s disease (PD). As stated earlier PD is a progressive neurodegenerative disease. This means that as of now PD CANNOT be cured. Once the disease begins it slowly but surely progresses. The rate of progression varies from patient to patient. While PD cannot be cured, there are a number of medications available which can control the symptoms of PD. At times the response with these medications is dramatic and very gratifying. A few salient points:
NOT every patient of PD needs to be treated. When PD initially begins the symptoms are usually mild and may cause minimal interference to the patient’s lifestyle. The mild tremor of PD might be dismissed by the patient as a mere nuisance. At this stage of the disease, the patient does not exhibit problems with his/her gait or balance. The rigidity, bradykinesia is not disabling. At this stage of the disease, the neurologist may opt to simply keep the patient under observation. The patient and the family are educated about the disease and instructed to remain in follow up (come for follow up appointments after very 3-4 months).
The most effective medication for the treatment of PD is LEVODOPA. Since PD is caused by deficiency of dopamine in the brain, the most effective way to treat it is to give dopamine from outside. So levodopa is administered in tablet form usually 3 times a day. Levodopa is combined with another chemical called carbidopa which helps to prevent the breakdown of levodopa in the stomach and thus ensures that high level of levodopa is absorbed and reaches the brain. This combination of LEVODOPA+CARBIDOPA is the main medication used to treat PD. LEVODOPA+CARBIDOPA combination tab is marketed by many different pharmaceutical companies under different names (Please check the common brand name of this combination in your country). The tablet is usually started at low dose three times a day. The neurologist then titrates the dose up based on clinical response and side-effects. The medication is usually well tolerated by most patients and the effect is gratifying. It is important to emphasize that this medication still remains the MOST effective medication for PD. LEVODOPA comes in many different formulations including now in an inhaled form. These formulations are prescribed as the disease advances. Please discuss the same with your neurologist.
DOPAMINE AGONISTS: is another class of medication commonly used to treat PD. As the name suggests medications in this class act by stimulating dopamine receptors in the brain. While not as effective as LEVODOPA+CARBIDOPA, dopamine agonists are commonly prescribed. Commonly used dopamine agonists include pramipexole (Mirapex), rotigotine (Neupro), and ropinirole (Requip). Some neurologists prefer to use a medication in this class as first line treatment and use LEVODOPA+CARBIDOPA when PD symptoms are more bothersome (PD is more advanced).
Amantadine is another medication used to treat PD. It is usually used in combination with either LEVODOPA+CARBIDOPA or DOPAMINE AGONISTS.
Anticholinergic drugs such as benztropine and trihexyphenidyl are also commonly used. These drugs are helpful in controlling symptoms such as tremor and muscle stiffness.
Drugs referred to as selective MAO B inhibitors such as selegiline are used by neurologists usually early in the disease course. There is limited evidence to suggest that medications in this class may be “neuroprotective”.
COMT inhibitors: another class of medications used in the treatment of PD.
Neurostimulator such as DEEP BRAIN STIMULATOR (DBS): A neurostimulator called DBS is sometimes implanted in PD patients. DBS is usually implanted in the brain of PD patients with advanced disease who are experiencing motor fluctuations, medication side-effects called dyskinesias and medication refractory tremor. Please discuss this further with your neurologist.
While medications form the cornerstone of treatment of PD, there are a number of other simple interventions which are very effective. It is important to remember that PD affects the motor system causing problems with gait and balance. Hence I make it a point to emphasize the importance of exercise to my patients and their family. Exercises which improve gait and balance are the most helpful.
Parkinson’s disease (PD) is a common neurological disease. This disorder of the brain is seen in people of all races and both sexes. PD is caused by the deficiency of a neurochemical called DOPAMINE in the brain. In this blog post I shall discuss the clinical presentation and diagnosis of PD.
Parkinson’s disease is included under the category of neurodegenerative brain disorders. What that means is that the disease is progressive. Once the disease starts, it slowly progresses. The rate of progression though varies from patient to patient. The disease onset is usually insidious. Most people first exhibit signs of the disease after age 60 (in some people the disease may start in the late 40’s or in their 50’s-this is then referred to as Early Onset Parkinson’s).
Disease onset-onset of PD is usually insidious and at times may not be noticed by the patient or the family. Typical first symptom may be a slight tremor (shaking) in the thumb of one hand/finger of one hand, the hand itself or the chin. The tremor is not disabling at onset and hence ignored by the patient/family. It is important to emphasize here that NOT ALL TREMORS ARE PD. There are numerous causes of tremor, many which are benign (do not signify any serious disease). PD tremor has some special characteristics (features) which helps to distinguish it from other types of tremors.
CHARACTERISTICS (FEATURES) OF PD TREMOR
The tremor is usually insidious in onset and of low amplitude.
The tremor is usually asymmetrical at onset (one thumb/one hand). As the disease progresses the tremor becomes more prominent and may involve both the sides of the body.
PD tremor is typically what is referred to as a RESTING TREMOR. What this means is that the tremor is most prominent when the hands are completely at rest (example-the tremor is noted when the patient’s hands are resting on his/her lap, resting on the driving wheel). This is an IMPORTANT distinguishing feature of PD tremor. Tremors which are more prominent when the hands are extended in front (POSTURAL TREMOR) or while in motion are usually not due to PD.
CLINICAL PRESENTATION OF PD (SIGNS AND SYMPTOMS)
PD initially presents with motor symptoms. Patients do not have sensory symptoms such as pain, numbness, tingling. The common motor symptoms of PD are the following:
Tremor: tremor of PD is a resting tremor (see above).
Bradykinesia: the word bradykinesia means “slowness of movement” and is one of the main symptoms of PD. The patient is slow to walk, slow to initiate movement. As PD progresses, the patient becomes more and more bradykinetic (slow). There is loss of spontaneous movements such as facial expressions, gesturing, eye blinks.
Rigidity: rigidity is another cardinal symptom of PD and refers to the stiffness which PD patients feel in their muscles. Rigidity can be detected by the neurologist on clinical examination.
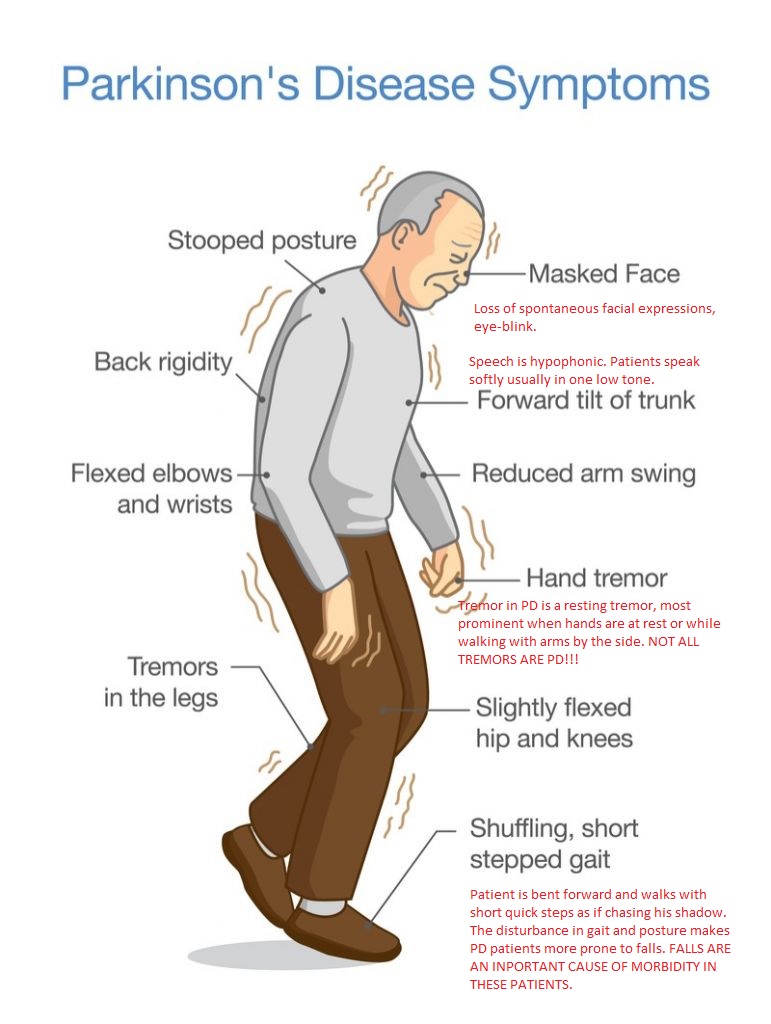
Disturbance of gait and posture: patients with PD experience a disturbance in their gait (how a person walks) and posture. A patient with PD is usually stooped (bent) forwards and walks with short quick steps. This is referred to as the SHUFFLING GAIT OF PD. This disturbance of gait and posture makes PD patients more prone to falls. It is important to emphasize here that FALLS ARE AN INPORTANT CAUSE OF MORBIDITY IN PD PATIENTS.
Photo source: *photo: https://www.labiotech.eu/medical/axovant-parkinsons-disease-gene/ (the above image has been edited)
DIAGNOSIS OF PD
The diagnosis of PD is predominantly clinical and has not changed much since the disease was first described by James Parkinson, an English surgeon in his now famous 1817 work AN ESSAY ON THE SHAKING PALSY.
PD is diagnosed in the following way:
Clinical examination by a neurologist: neurologists are able to diagnose PD after taking a history and doing a neurological examination in which they assess for tremor, bradykinesia, rigidity and gait/posture.
Neuroimaging: it is important to emphasize that neuroimaging studies such as CT scan head and MRI brain are usually reported normal in patients with PD.
New imaging modalities: DaT scan is a new imaging test which uses a small amount of a radioactive tracer drug to determine how much dopamine is available in a patient’s brain. It is important to emphasize that DaT scan is neither needed nor a definitive test for PD diagnosis. It is primarily helpful in differentiating Parkinson like diseases (Parkinsonian syndromes) from a more benign condition called essential tremor (ET).
DISCLAIMER: The information in this blog is for educational and informational purposes only. It does not constitute medical advice. Use of the site content does not establish any patient-doctor relationship. If you choose to write to me or post a comment on this blog, please do not divulge any personal medical information.













{kind=link}
{kind=link}
{kind=link}
You must be logged in to post a comment.