Parkinson’s disease (PD) is a common neurological disease. This disorder of the brain is seen in people of all races and both sexes. PD is caused by the deficiency of a neurochemical called DOPAMINE in the brain. In this blog post I shall discuss the clinical presentation and diagnosis of PD.
Parkinson’s disease is included under the category of neurodegenerative brain disorders. What that means is that the disease is progressive. Once the disease starts, it slowly progresses. The rate of progression though varies from patient to patient. The disease onset is usually insidious. Most people first exhibit signs of the disease after age 60 (in some people the disease may start in the late 40’s or in their 50’s-this is then referred to as Early Onset Parkinson’s).
Disease onset-onset of PD is usually insidious and at times may not be noticed by the patient or the family. Typical first symptom may be a slight tremor (shaking) in the thumb of one hand/finger of one hand, the hand itself or the chin. The tremor is not disabling at onset and hence ignored by the patient/family. It is important to emphasize here that NOT ALL TREMORS ARE PD. There are numerous causes of tremor, many which are benign (do not signify any serious disease). PD tremor has some special characteristics (features) which helps to distinguish it from other types of tremors.
CHARACTERISTICS (FEATURES) OF PD TREMOR
- The tremor is usually insidious in onset and of low amplitude.
- The tremor is usually asymmetrical at onset (one thumb/one hand). As the disease progresses the tremor becomes more prominent and may involve both the sides of the body.
- PD tremor is typically what is referred to as a RESTING TREMOR. What this means is that the tremor is most prominent when the hands are completely at rest (example-the tremor is noted when the patient’s hands are resting on his/her lap, resting on the driving wheel). This is an IMPORTANT distinguishing feature of PD tremor. Tremors which are more prominent when the hands are extended in front (POSTURAL TREMOR) or while in motion are usually not due to PD.
CLINICAL PRESENTATION OF PD (SIGNS AND SYMPTOMS)
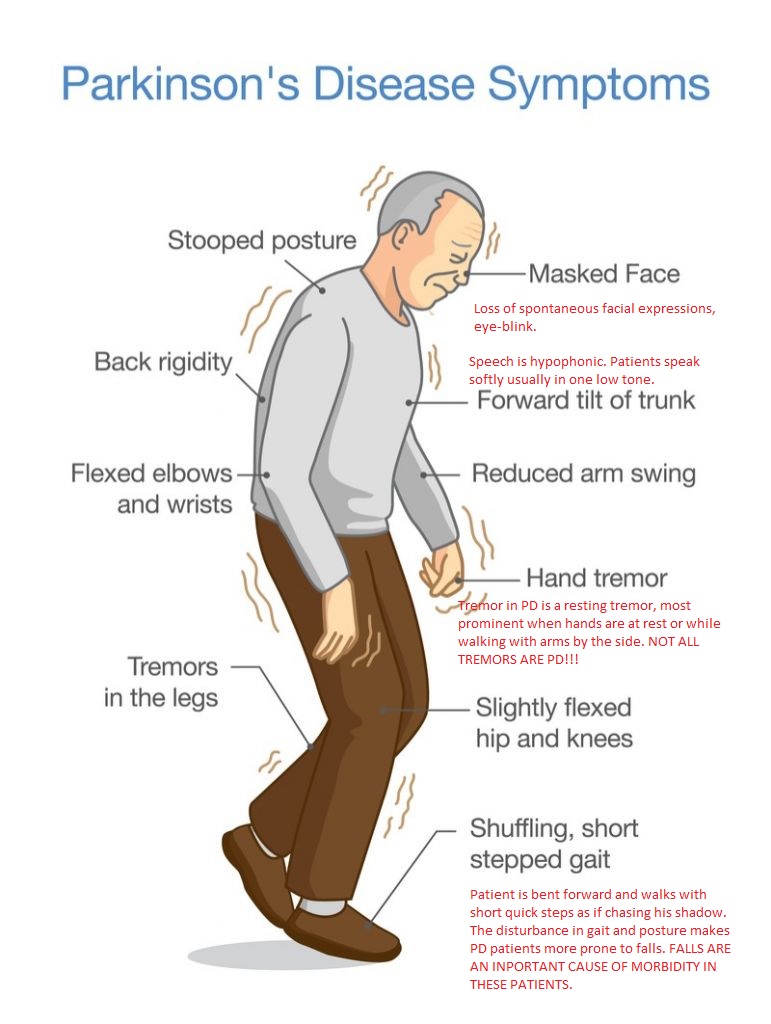
PD initially presents with motor symptoms. Patients do not have sensory symptoms such as pain, numbness, tingling. The common motor symptoms of PD are the following:
- Tremor: tremor of PD is a resting tremor (see above).
- Bradykinesia: the word bradykinesia means “slowness of movement” and is one of the main symptoms of PD. The patient is slow to walk, slow to initiate movement. As PD progresses, the patient becomes more and more bradykinetic (slow). There is loss of spontaneous movements such as facial expressions, gesturing, eye blinks.
- Rigidity: rigidity is another cardinal symptom of PD and refers to the stiffness which PD patients feel in their muscles. Rigidity can be detected by the neurologist on clinical examination.
- Disturbance of gait and posture: patients with PD experience a disturbance in their gait (how a person walks) and posture. A patient with PD is usually stooped (bent) forwards and walks with short quick steps. This is referred to as the SHUFFLING GAIT OF PD. This disturbance of gait and posture makes PD patients more prone to falls. It is important to emphasize here that FALLS ARE AN INPORTANT CAUSE OF MORBIDITY IN PD PATIENTS.
DIAGNOSIS OF PD
The diagnosis of PD is predominantly clinical and has not changed much since the disease was first described by James Parkinson, an English surgeon in his now famous 1817 work AN ESSAY ON THE SHAKING PALSY.
PD is diagnosed in the following way:
- Clinical examination by a neurologist: neurologists are able to diagnose PD after taking a history and doing a neurological examination in which they assess for tremor, bradykinesia, rigidity and gait/posture.
- Neuroimaging: it is important to emphasize that neuroimaging studies such as CT scan head and MRI brain are usually reported normal in patients with PD.
- New imaging modalities: DaT scan is a new imaging test which uses a small amount of a radioactive tracer drug to determine how much dopamine is available in a patient’s brain. It is important to emphasize that DaT scan is neither needed nor a definitive test for PD diagnosis. It is primarily helpful in differentiating Parkinson like diseases (Parkinsonian syndromes) from a more benign condition called essential tremor (ET).
DISCLAIMER: The information in this blog is for educational and informational purposes only. It does not constitute medical advice. Use of the site content does not establish any patient-doctor relationship. If you choose to write to me or post a comment on this blog, please do not divulge any personal medical information.
Nitin K Sethi, MD, MBBS, FAAN

You must be logged in to post a comment.