
Boxing drills for Parkinson’s disease patients (please do under supervision)
Please remember patients with PD are prone to falls. If you or your loved one with PD decides to do some of these drills to help improve gait, balance and stance, please do them under the close supervision of a physical therapist or a trained boxing instructor.

Parkinson’s disease (PD) is a common neurological disease. This disorder of the brain is seen in people of all races and both sexes. PD is caused by the deficiency of a neurochemical called DOPAMINE in the brain. In this blog post I shall discuss the clinical presentation and diagnosis of PD.
Parkinson’s disease is included under the category of neurodegenerative brain disorders. What that means is that the disease is progressive. Once the disease starts, it slowly progresses. The rate of progression though varies from patient to patient. The disease onset is usually insidious. Most people first exhibit signs of the disease after age 60 (in some people the disease may start in the late 40’s or in their 50’s-this is then referred to as Early Onset Parkinson’s).
Disease onset-onset of PD is usually insidious and at times may not be noticed by the patient or the family. Typical first symptom may be a slight tremor (shaking) in the thumb of one hand/finger of one hand, the hand itself or the chin. The tremor is not disabling at onset and hence ignored by the patient/family. It is important to emphasize here that NOT ALL TREMORS ARE PD. There are numerous causes of tremor, many which are benign (do not signify any serious disease). PD tremor has some special characteristics (features) which helps to distinguish it from other types of tremors.
CHARACTERISTICS (FEATURES) OF PD TREMOR
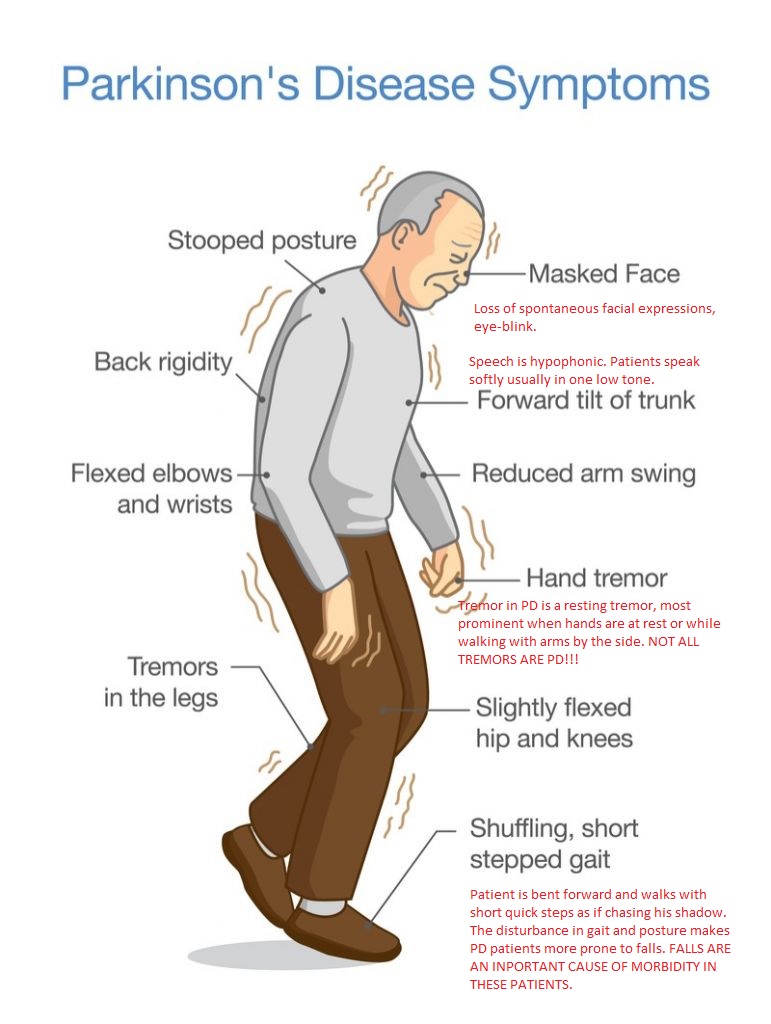
CLINICAL PRESENTATION OF PD (SIGNS AND SYMPTOMS)
PD initially presents with motor symptoms. Patients do not have sensory symptoms such as pain, numbness, tingling. The common motor symptoms of PD are the following:
DIAGNOSIS OF PD
The diagnosis of PD is predominantly clinical and has not changed much since the disease was first described by James Parkinson, an English surgeon in his now famous 1817 work AN ESSAY ON THE SHAKING PALSY.
PD is diagnosed in the following way:
DISCLAIMER: The information in this blog is for educational and informational purposes only. It does not constitute medical advice. Use of the site content does not establish any patient-doctor relationship. If you choose to write to me or post a comment on this blog, please do not divulge any personal medical information.
Nitin K Sethi, MD, MBBS, FAAN
Is aging normal or abnormal/pathological? No one quite knows the answer to that question. What we do know is that as we age, neurological disorders become increasingly common. These may range from well defined neurodegenerative diseases like Alzheimers dementia, Parkinson disease and amyotophic lateral sclerosis to other less well defined conditions like gait disorders, “balance problems”, “forgetfulness and senior moments” and increased propensity to falls. Strokes become more common in the aged brain vessels.
As life expectancy increases and more and more people live past the eight decade, neurological conditions become common and account for substantial morbidity and mortality in the oldest old (above 85). Earlier when the life expectancy was in the 60s, we did not see so much Alzheimers dementia, Parkinson’s disease or brain tumors. People died of other “natural” and “unnatural” causes before the brain showed clinical manifestations of neurodegeneration.
Is it the norm that as we age, a substantial majority of us are destined to develop dementia? Clinical studies have clearly shown that Alzhemier disease pathology increases with age and the incidence of the disease becomes increasingly common as one goes past 85 (the oldest old). Other studies suggest that though not all the oldest old show clinical dementia, a substantial majority have cognitive difficulties if carefully tested for at the bedside.
Why do neurological conditions become more “common” as we age and can we do anything to alter this? Many theories have been propounded. Increased amyloid deposition in the brain has causal association with Alzheimers dementia, in the same vein deposition of iron in the basal ganglia has been postulated to cause various basal ganglia pathology. There is increased oxidative stress in the “aged” brain which leads to free radical formation and damage to the cellular DNA. Genes get switched off or on triggering the disease process. A lot still needs to be learned about the neurology of aging.
While the mechanisms are still been elucidated, is there anything which we can do to change our “risks”. In the absence of good studies most of the data is open to interpretation. Aspirin prophylaxis, modification of microvascular and macrovascular risk factors like hypertension, diabetes mellitis and dyslipidemia (high “bad” cholesterol) all seem to be reasonable interventions. Obesity and sedentary life styles are bad for the brain too. Regular physical as well as brain exercises (neurobics) keeps the brain healthy and increases neuronal reserve. The role of anti-oxidants like coenzyme Q10 and alpha lipoic acid is still been defined. As they are relatively innocuous and free from side-effects, I would recommend them on a case by case basis. Episodes of major depression “hurt” the brain and aggressive treatment with anti-depressants should be initiated early rather than late.
The neurology of aging remains an uncharted territory but there is hope yet.
Nitin Sethi, MD

You must be logged in to post a comment.