Nitin K Sethi, MD, MBBS, FAAN
sethinitinmd@hotmail.com

Epilepsy is a common neurological condition in which patients suffer recurrent seizures (also referred to as convulsions).
A generalized convulsion is a rather dramatic event. If it occurs while the patient is standing, frequently the patient gets no warning and falls down striking the ground hard. This is the time injuries occur. As the patient is falling down, he/she is amnestic for the entire episode. Family/bystanders notice that initially the patient stiffens (arms and legs are extended, eyes are rolled up into the head, clenching of the teeth occurs which at times leads to the tongue getting bitten, the patient may at times suffer loss of bladder control). This “tonic” phase is followed by the “clonic” phase during which convulsive movements occur. The seizure stops in a minute or two but the patient remains unresponsive and slowly regains consciousness.
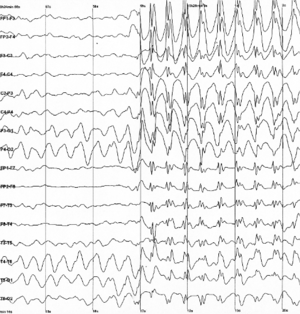
If the above convulsion occurs WHILE the patient is undergoing an EEG test (electroencephalogram), the abnormal brain activity is picked up by the test (see example below) and the diagnosis confirmed.
Based on the misfiring recorded on the EEG, the neurologist can then opine what kind of epilepsy the patient has and where (which part) in the brain the seizures are originating from.
WHEN A SEIZURE IS NOT A SEIZURE–LET US TALK ABOUT PSEUDOSEIZURES
Pseudoseizure is the term used for events that appear to be epileptic seizures but, in fact, are not. So while the patient may have a dramatic event where in he/she shakes, may roll up the eyes, arch his back, moan, make noises and vocalize, THERE IS NO ABNORMAL EXCESSIVE SYNCHRONOUS CORTICAL ACTIVITY (meaning that on the EEG, the brain waves appear normal without any misfiring).
Pseudoseizures are referred to by various names such as psychogenic non-epileptic events (PNES), non epileptic events (NEE), non epileptic seizures, hysterical seizures.
When pseudoseizures are suspected, a neurologist or epileptologist (epilepsy specialist) shall take a detailed history, may order a MRI scan of the brain and then attempt to capture one of these events on VIDEO-EEG MONITOR (Video-EEG is a special kind of EEG in which simultaneous EEG and video recording of the patient is carried out). The goal is to capture one of the patient’s reported events on video-EEG. If no misfiring of the brain is observed during the event, a diagnosis of pseudoseizures is made.
The non-epileptic (“YOU DO NOT HAVE EPILEPSY” OR “THESE ARE NOT SEIZURES”) nature of the events is then explained to the patient and the family and an attempt is made to try to determine the underlying cause (Why is the patient having these events?). There are many causes of pseudoseizures such as mental stress, sexual or physical abuse, personality disorders, dissociative disorders, affective disorders (mood disorder, anxiety, depression), substance abuse disorder, family conflict, conflict or stress at work, problems in marriage among others.
The treatment is usually a combination of psychotherapy and use of medications (selective serotonin reuptake inhibitors). With support and understanding most patients start to improve and the events either stop completely or become less frequent.

You must be logged in to post a comment.