Nitin K Sethi, MD, MBBS, FAAN
sethinitinmd@hotmail.com
Background
American football, soccer, rugby, ice hockey, boxing, mixed martial arts, and wrestling are popular contact and combat sports both in the United States and in countries around the world. In these sports head impact exposures resulting in concussions are common. In American football, rugby and soccer, concussive injuries to the brain occur accidently when there is contact of the player’s head with the opposing player(s) head, torso, turf or as occurs in soccer with the ball while heading. In boxing every punch thrown at the head is thrown with the intention of winning by causing a knockout. As a result, concussions, and acute traumatic brain injuries such as subdural and epidural hematoma are common. Subdural hematoma is the most common cause of boxing related mortality. In recent years, the risk of chronic traumatic encephalopathy (CTE), a chronic neurodegenerative disorder associated with contact and combat sports has garnered the attention of physicians, players, and fans.
Concussion definition and evaluation
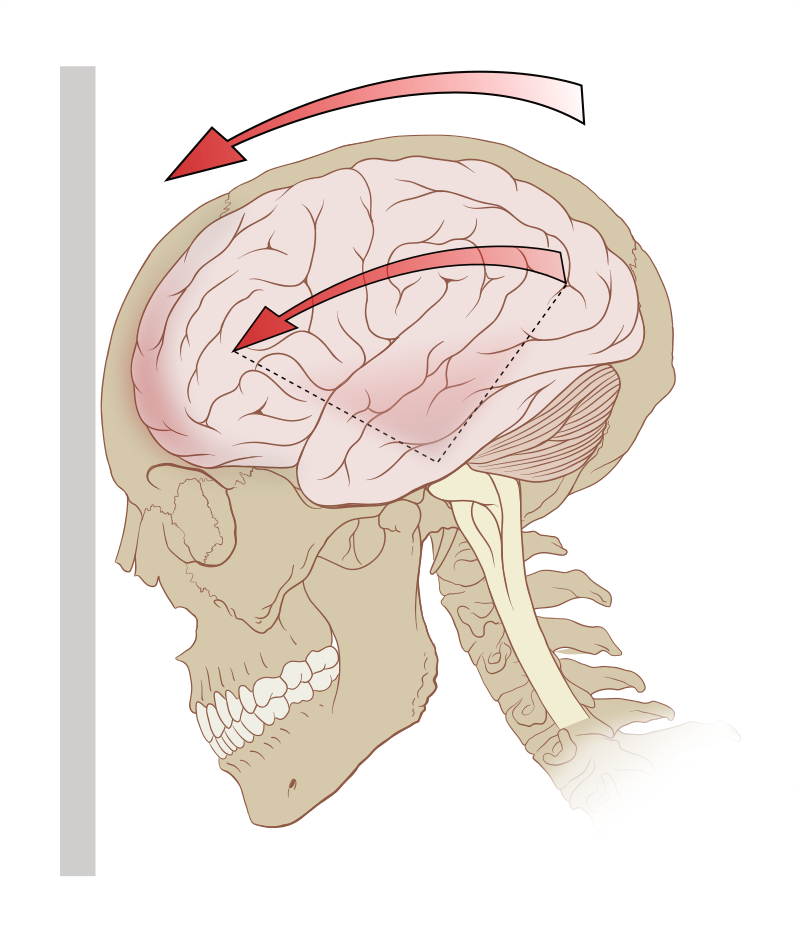
Concussion is defined as a clinical syndrome characterized by immediate and transient alteration in brain function, including alteration of mental status and level of consciousness, resulting from mechanical force or trauma. It is important to remember that loss of consciousness is not required for a concussion. Concussions are informally and non-scientifically graded into mild, moderate, and severe based on the duration of loss of consciousness and post traumatic amnestic period. Concussive properties of any head impact exposure depend upon the force, velocity, and angle of the hit to the cranium and how the mechanical forces are transferred and absorbed through the intracranial cavity. Both linear and rotational (angular) acceleration forces play a role as does impact deceleration occurring when the athlete falls and strikes the head against the ground.
The nature of many contact and combat sports is such that head impact exposures cannot be altogether avoided. Abundant medical literature highlights the long-term health significance of multiple head impact exposures. Minor concussions (sub concussive injuries) contribute to the development of CTE, a neurodegenerative disorder presenting with a constellation of cognitive, mood, and behavioral changes along with motor system dysfunction (Parkinsonism) usually after the athlete has retired. The symptoms of concussion are predominantly subjective such as headache, dizziness, nausea, light sensitivity, sound sensitivity, and cognitive dysfunction. Frequently, when athletes sustain head impact exposures, they themselves are unaware that they are concussed and continue to play. As a result, it is important that when an athlete sustains a head impact exposure, a standardized concussion evaluation be conducted. While this can be conducted on the sidelines, evaluation in the locker room where the athlete is less likely to be distracted is more ideal. Since some athletes exhibit motor signs such as impaired coordination, balance, and stance after a concussion while others exhibit only cognitive dysfunction, it is important that multimodal concussion evaluation be conducted. This includes use of Maddocks questions to gauge awareness, standardized concussion assessment tools such as SCAT5, King Devick test and Balance Error Scoring System (BESS).

Management of concussive injury
The athlete’s mentality is to never quit. Hence many athletes will deny symptoms of a concussive injury to the brain. Physicians should be aware of this. An athlete who has suffered a concussion should be pulled out of play and “benched.” This is done for two main reasons. A concussed athlete with impaired attention, concentration, balance, and coordination is more prone to a second head impact exposure. The other reason is that if the concussed athlete continues to play, it is likely that he or she will exhibit more profound and prolonged post-concussion symptoms. The benched athlete is advised a period of cognitive and physical rest. The rationale for this is that a concussed brain is in a state of energy crises and fares better when the cognitive and physical demands on it are less. Cognitive rest entails pulling back from cognitive activities such as team meetings, college work, screen time (amount of time spent using devices with screens such as a smartphone, computer, television, or video game console). Physical rest entails pulling back from normal physical activities such as running and jogging. Here it is important to emphasize that complete cocooning is ill-advised with recent research work showing that it may in fact be detrimental and lead to prolongation of symptoms. The concussed athlete should be evaluated by a physician skilled in concussion management. In most cases neuroimaging with computed tomography or magnetic resonance imaging is not warranted and if conducted comes back negative. There is currently no validated imaging or biofluid (blood or cerebrospinal fluid) biomarkers for concussion. In the absence of biomarkers, the diagnosis of concussion is made clinically based on history of head impact exposure followed by characteristic symptoms (post-concussion symptoms). The concussed athlete is advised to drink adequate water and to avoid alcohol intake and sudden inversions till symptomatic. The role of supplements such as magnesium, vitamin B2 (riboflavin), vitamin B12, fish oil among other remains unclear but these are frequently prescribed. There is no treatment for the head injury itself. Treatments for symptoms of concussion such as headache, dizziness, cognitive impairment, poor sleep, mood, and behavioral disorder involves a multi-disciplinary team consisting of neurologists, neuropsychologists, neurosurgeons, neuroradiologists, neuro-ophthalmologists, physical therapists, occupational therapists, and vestibular therapists with expertise in concussion management.
After a few days of cognitive and physical rest when the acute concussion symptoms have abated, the athlete begins a graded and gradual return to play (RTP) program preferably under the guidance of an athlete trainer with expertise in concussion management. Nowadays most contact and combat sports have sport specific return to play (RTP) protocols. Despite individual variations, the basis tenant remains the same and involves the athlete progressing from light aerobic activity (walking or stationary bike for 10 minutes, no resistance training) to sport-specific activity/drills to non-contact training drills to contact practice and if asymptomatic return to play after a release has been signed by the treating physician.
Conclusion
Concussion is a common head injury in contact and combat sports. Timely identification of the concussed athlete, removal from play and medical management usually results in a good outcome. Closer medical supervision of sports and education of all concerned parties on concussion recognition and management remains the need of the hour.

{kind=link}
You must be logged in to post a comment.