It is the start of the New Year and I want to begin by wishing all the readers of my blog a very happy and healthy New Year 2013. May you all be blessed with not only a healthy brain but also a healthy mind!.
I decided that my first post in the New Year 2013 should be on strokes and more importantly on how to recognize a stroke in a timely fashion and how to prevent it. After all a stroke prevented is a brain saved.
So let us begin without delay. Keeping things simple the best way to describe a stroke is to compare it to a heart attack. A heart attack occurs when one of the main arteries of the heart suddenly gets blocked. The sudden lack of blood flow leads to ischemia of the heart (basically the part of the heart supplied by that blood vessel does not get blood/oxygen and if the blocked artery is not opened/ recanalized in time irreversible death of cardiac muscle/tissue occurs). Something similar happens during a stroke and hence sometimes strokes are referred to as brain attacks. A blood vessel in the brain either gets blocked (ischemic stroke) or ruptures (hemorrhagic stroke) and if not opened in time the part of the brain supplied by that blood vessel perishes. The signs and symptoms of the stroke depend upon which part of the brain is involved.
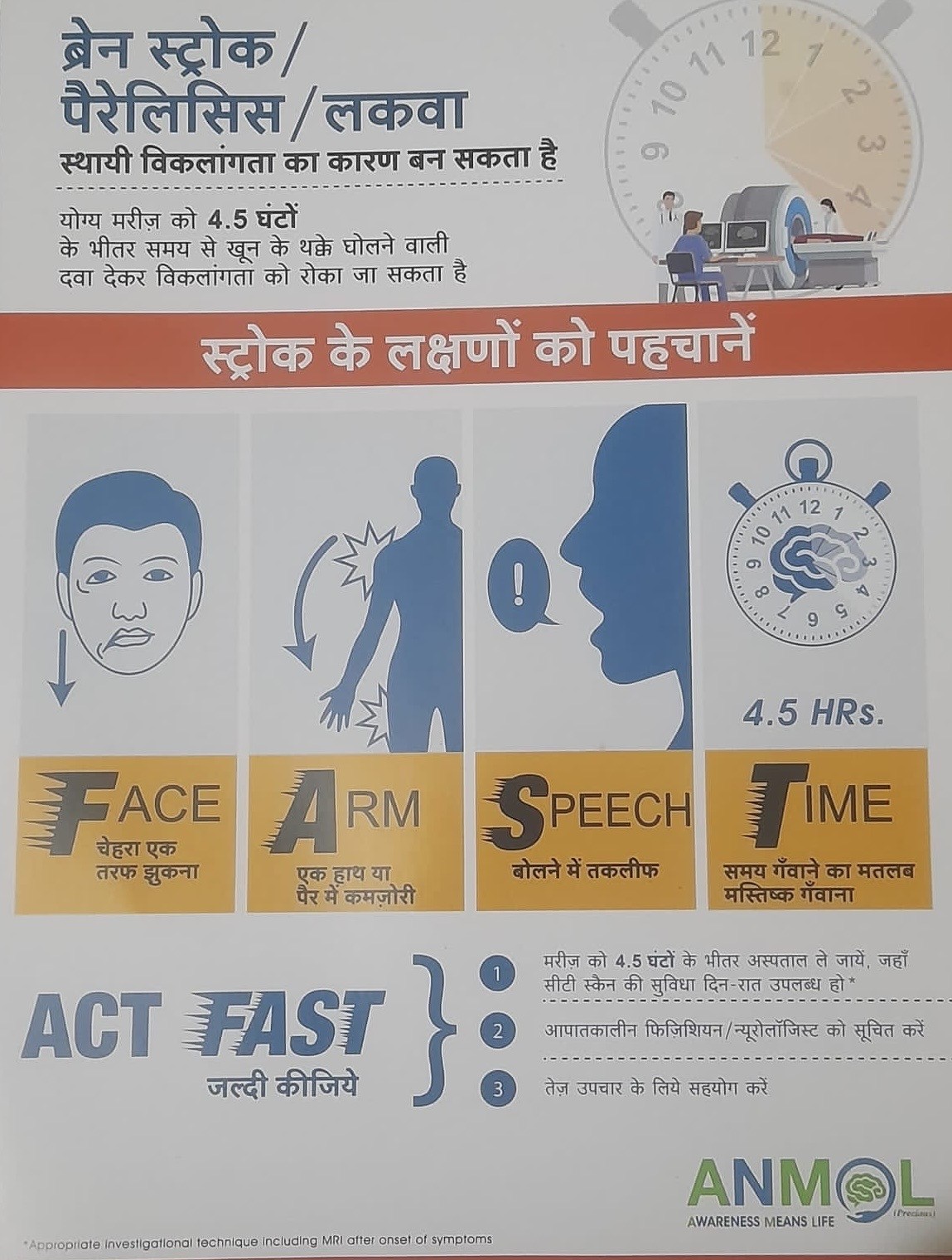
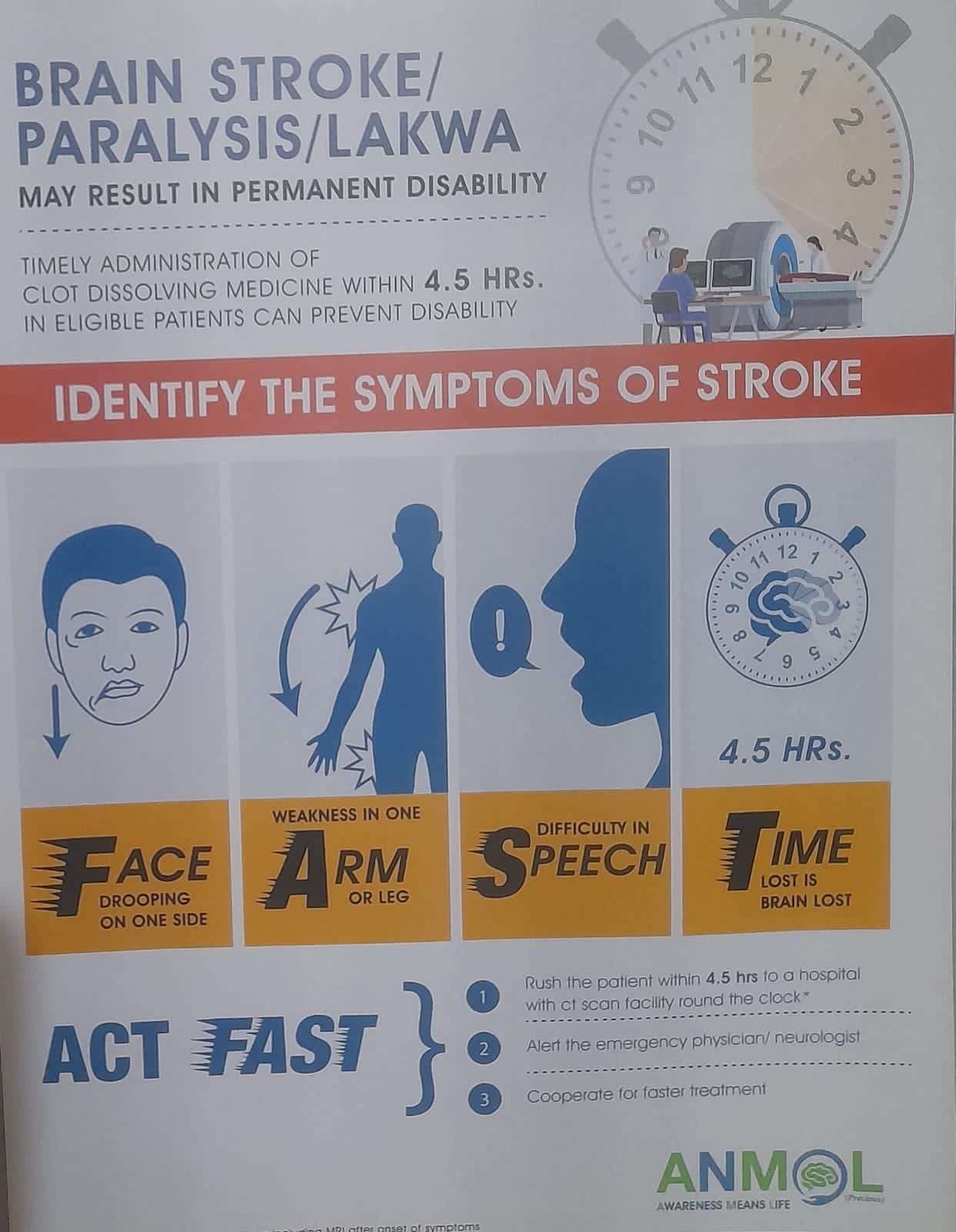
Warning signs of a stroke:
1. Sudden onset of weakness in the arm and leg on one side of the body (for example abrupt onset of motor weakness in the right arm and leg usually indicates ischemia/lack of blood flow or hemorrhage involving the left side of the brain). That said strokes may be more subtle or unusual in their presentation–weakness in only one arm or one leg, weakness in one arm and contralateral face and so forth.
2. Sudden onset of numbness (loss of sensation but no marked weakness) on one side of the body. Again presentation may be more unusual–abrupt onset of numbness one side of face or just in one arm.
3. Sudden onset of vision problems–double vision or loss of vision in one eye or loss of vision in one half/part of visual field.
4. Sudden onset of difficulty walking or balance–unable to walk in a straight line, dizziness (not all dizziness is stroke though).
5. Sudden onset of speech difficulty–either unable to speak (words are mumbled, not clear, language difficulty), unable to comprehend speech.
6. Sudden onset of complete loss of hearing in one ear (rare form of stroke).
7. Sudden onset of a combination of the above symptoms-usually this is the case.
One of the major problems with stroke is that frequently the symptoms and signs are very subtle and may be ignored by the patient and his family/friends. By the time the patient seeks medical attention, the stroke is already completed (remember when it comes to stroke–TIME IS BRAIN) and the damage is already done. In the case of a heart attack the signs are hard to ignore–sudden onset of squeezing chest pain along with sweating and a sinking sensation. Patients are forced to go to the hospital and seek attention. On the other hand the brain is far more quieter when it suffers a brain attack–no pain, no sweating just quiet suffering of the ischemia.
So what to do when you or someone close to you is suffering a stroke? The most important thing is not to delay seeking attention. You can only be helped if you reach the hospital in a timely fashion ideally within the first hour to 90 minutes of the stroke. So seek attention at once. It is better to reach the hospital and be told that you misread your symptoms and did not suffer a stroke rather than reach late when nothing can be done to help you apart from supportive care.
So let us start the New Year 2013 by preventing strokes. Remember your brain is your best friend. Protect him, nourish him, take care of him.
Nitin K Sethi, MD
I had a stroke like episode—what do I do?
Nitin K Sethi, MD
Assistant Professor of Neurology
New York-Presbyterian Hospital
Weill Cornell Medical Center
New York, NY 10065
I frequently see patients admitted to the hospital for evaluation of a suspected stroke like episode. Most of these patients are “normal” with no neurological signs and symptoms (the presenting symptom has invariably resolved by the time of their admission to an acute care facility).
So what are these stroke like episodes which scare patients and doctors alike leading to admission to a hospital and invariably a battery of tests including but not limited to MRI scans of the brain? Well some may be as vague as an episode of sudden dizziness, difficulty walking or weakness in the arms and legs, others are more restricted-an episode of difficulty speaking (I could speak but my words did not come out right or my speech was slurred as if I was drunk), loss of vision in an eye and so on.
When patients present to the ER or a doctor’s office with a history of such symptoms, they are frequently advised admission to rule out a possible stroke. When people think of stroke, they usually think of someone with weakness of the arm and leg but stroke signs and symptoms can be more subtle. Many patients have what we refer to as transient ischemic attacks (TIAs) prior to the stroke. As the name suggests, TIAs are transient (short lived) episodes of ischemia to the brain. Let me try to explain a TIA with the aid of an example. Let us assume a clot (entangled platelets and cholesterol crystals) breaks from the heart and goes up to the brain via the carotid artery (the carotid artery is one of the main arteries carrying blood to the brain). As it goes up further and further, it may get lodged in the ophthalmic artery (the ophthalmic artery is a branch of the carotid artery and supplies the retina of the eye). Now if the ophthalmic artery gets blocked by the clot there is no blood supply to the retina with resulting loss of vision in that eye (patients frequently complain of a black curtain descending in front of their eye). If the clot breaks by itself and dissolves the vision comes back (we call this transient monocular blindess—transient blindness in one eye). There you have suffered a transient ischemic episode.
There can be other types of TIAs which can involve different blood vessels in the brain and present with a myriad of signs and symptoms such as dizziness, double vision and difficulty speaking. So what is so important about TIAs?
Well put in simple language a TIA may be a warning sign of a future stroke (and by future, I mean in the NEAR future). It is a sign that all is NOT well with the blood vessels of the brain or the heart (either the vessels are slowing getting narrowed or the heart is not functioning well and throwing up small blood clots into the brain). TIAs thus should be aggressively and thoroughly investigated.
What are the stroke risk factors?
How can they be modified?
Does the patient need to be on any blood thinners?
As I frequently explain to my patients and their families
“A TIA IS A CRY OF THE BRAIN, A CRY FOR HELP
IF YOU DO NOT HEED IT IN TIME
YOU RISK HAVING A DEVASTATING STROKE IN THE NEAR FUTURE”
Just received this from an unknown reader. Just goes to show how the onset of Bell’s palsy might be subtle and patient’s frequently think they may be having a stroke.
Personal Regards,
Nitin Sethi, MD
A patient’s story follows…..
well i am on my first full day and my storie goes like this.
starting yesterday at about 7:30 am I started to learn a new appreciation for life. It all started on Saturday night I felt a sinus headache coming on and later a pain in the left side of my neck & ear. I then proceeded to get a few Excedrin and a cup of hot coffee. I had a great time at a Halloween party that night woke up on Sunday felt fine other than a little sinus pressure. So I proceeded to take some Tylenol multi symptom sinus medicine which I rarely take because I hate man made drugs! Went to bed woke up Monday and felt some pressure in my left side of my face, had some breakfast, kissed the wife and kids goodbye and was off to my hour drive down to West Palm Beach. Got to work and felt a little sleepy, I ended up sleeping for like the first hour at work. Then sally called me up to the front office for something and when I got there she said “what is wrong with your face” of course I laughed and said “nothing more than normal why is it killing you LOL” she said
no your left eye looks weird and your face looks swollen . Well to cut it shout I was having a severe allergic reaction to the Tylenol multi-symptom medicine. So I called the doc and they said to take some Benadryl, so I did. Shortly after I noticed I started to have a numbing in my left side of my face. I could not close my left eye by its self and when I took a drink of water it streamed down the left side of my face. I went to the mirror to find that the left side of my face was droopy and is seemed to be paralyzed. I was freaking out by now of course thinking I was having a stroke. I went to the doctor and found out that between a pinched nerve in my neck that was a result of a dislocating rib under my shoulder blade and a Sinus infection I had damaged my 7th cranial nerve resulting in a condition called Bell’s palsy.
Thrombolysis for stroke- sooner the better!!!
Nitin K.Sethi, MD
A new study on treatment of stroke was published this week in the New England Journal of Medicine (NEJM). The study concerns thrombolytic therapy for stroke and since I feel very strongly about stroke prevention and treatment, I thought I would share the relevant details with my readers. The study “Thrombolysis with Alteplase 3 to 4.5 hours after acute ischemic stroke” and the accompanying editorial by Dr. Lyden appears in the Sep 25th issue of NEJM.
Ischemic stroke (stroke due to lack of blood flow to the brain) can be devastating leaving survivors with neurological deficits (paralysed on one half of the body, unable to walk or talk). When a patient lands up in the ER with an acute ischemic stroke (I like to refer to it as “brain attack” kind of similar to “heart attack” which patients and family members find easier to understand), as doctors we try hard to salvage the brain tissue at risk of “death”. One of the main drugs in our armament in this fight is a drug called tPA (Tissue plasminogen activator). tPA acts like a clot buster (the drug lyses/ bursts the clot in the brain and helps to reestablish blood flow).
Let me try to explain this in a more simple way. A blood clot breaks from the heart and travels up to the brain, there it lodges in a small blood vessel of the brain preventing blood flow distally (beyond the clot). Patient presents with left arm and leg weakness to the hospital. The brain tissue supplied by the blocked blood vessel now gets no blood and starts to die. “A STROKE IN EVOLUTION” . If blood flow is not reestablished soon, the brain tissue suffers irreversible necrosis and death. This patient is given tPA, the drug lyses/ bursts the clot and helps to reestablish blood flow. The patient who was weak on one side starts moving his arm and leg again.
It is not as simple as I made it out to be above. Patients have to meet strict inclusion criteria before tPA can be administered. Also the drug has a window period and has to be given intravenously within 3 hours of the stroke starting. 3 HOURS THAT IS THE GOLDEN PERIOD. Patients presenting to the ER after 3 hours are usually denied tPA for 2 main reasons-one the tissue which was at risk for stroke is now irreversibly destroyed and thus cannot be salvaged and second the risk for intracranial hemorrhage (bleeding inside the brain) is high.
The study reported in NEJM extends this window period (golden period) from 3 to now 4 and half hours. You can now understang why this study is generating so much interests among doctors and neurologists in particular. Patients presenting to the hospital upto 4 and half hours after an ischemic stroke can be given tPA provided they meet the other inclusion criteria (and none of the exclusion criteria).
But as Dr. Lyden in his editorial rightly points out, this should not be taken to mean that now you have more time to wait before going to the hospital to seek help (or for us doctors as more time to wait before we decide to administer tPA). When it comes to stroke, TIME IS BRAIN. The more you wait, the more brain tissue is lost, the more brain cells die, the more disability the patient is left behind with.
It is extremely important that the public learn to recognize the early warning signs of stroke and seek help as soon as possible. You can read more about the early warning signs of stroke either on my blog here or on my website http://braindiseases.info.
Salt and stroke: what is the connection?
Nitin K Sethi, MD
I recently read an editorial written by Norman Campbell and David Spence on “Stroke prevention and sodium restriction” in the Canadian Journal of Neurological Sciences in which they talk about the effect of dietary sodium restriction on the incidence of stroke. As we all know stroke prevention is a much more cost effective strategy as compared to treatment of acute stroke. Unfortunately more attention is being paid to treatment and management issues surrounding acute stroke and precious little to the prevention of stroke. I strongly feel that for every 1 lecture which a neurologist gives about treatment of acute stroke, he should give 10 lectures about the prevention of stroke.
Restriction of dietary sodium or rather salt in the diet is one such cost-effective strategy to prevent strokes. Increased salt in the diet raises the blood pressure and blood pressure is the number one risk factor for strokes. The authors make a strong point for government legislation to cut down the amount of salt added to processed foods or that eaten in restaurants. As they rightly say advise to patients to reduce salt intake is by itself relatively ineffective because sodium (salt) sources are ubiquitous and not apparent to the consumer. You may not add any salt to your diet when you cook at home but salt is added to nearly every food item at the time of processing. It is only by government legislation and action that salt content of food items can be lowered. Low salt content shall help in lowering blood pressures and thus prevent cardiovascular and cerebrovascular events (heart attacks and brain attacks!!!)
So watch the salt in your diet everyone. Remember a stroke prevented is a brain saved!!!
I want to lay stress on the warning signs of a stroke. We all need to be aware of these as a stroke can strike anyone anywhere and with stroke time is brain. The sooner the stroke is recognized and help is sought the better is the outcome.
So let us get to the heart of the topic. The following are some of the warning signs of an impending stroke/ stroke in evolution:
1) Sudden onset of speech difficulty. Either unable to speak or unable to comprehend speech (the patient can speak but cannot understand, so whatever he speaks makes no sense. We call this jargon speech). At times the problem with language can be more subtle: unable to name things (we call this nominal aphasia or anomia), the speech is slurred (we call this dysarthia).
2) Sudden onset of weakness in one arm or leg usually of the same side. For example weakness in right arm and right leg or in the left arm and left leg. This weakness may be prominent and the patient may not be able to move the arm and leg at all or it may be more subtle.
3) Sudden onset of numbness in one arm or leg usually of the same side. Numbness is hard to define and patients may use words like “weakness”, “tightness”, “dead feeling” or “my one side feels as if I slept on it”.
4) Sudden onset of facial weakness. One side of the face usually starts to sag, the smile is crooked when the patient attempts to smile and the patient may drool from the angle of the mouth.
5) Sudden onset of gait problems: the patient is unsteady and falls when attempting to walk. The balance is off. Patient is clumpsy and appears “drunk”.
6) Sudden onset of visual problems: patient may have an episode of transient loss of vision in one eye ( I felt as if a curtain decended in front of my eye). We call this transient monocular blindness and this is a TIA (transient ischemic attack). Patients may also complain of a field cut (unable to see one part of the visual field).
7) Acute loss of hearing in one ear especially in the elderly (this is a rare sign of a stroke).
Nitin Sethi, MD
Today I was having dinner when a friend asked me ” how can I reduce my risk of stroke?”. Briefly he explained to me that he had 2 heart attacks in the past. At that time he was found to have “slightly” high blood pressure and “bad” cholesterol. He said he was talking 2 medicines to lower his blood pressure and one to bring down his cholesterol. He could not provide me with further details and again I was suprised how little some of us know about our own medical condition. If I had asked him how his car was doing, I am sure he would have been able to furnish me a ton of detail. The mileage, the last oil change date, the date when the next oil change was due would have come rolling out.
Why do we neglect our own health? Is it just something we are not comfortable in talking about. Like a bad dream which one day when we wake up we shall not have to deal with any more. Some patients have inherent faith that God is watching out for them. This is particularly true in some cultures like for example in India, where some people feel that everything is God’s will. Hence they either detest taking medications or feel they do not need to take them. Some are lax with their follow up appointments. Other shall take the blood pressure and cholesterol lowering medications, only to self discontinue them when their blood pressure and cholesterol becomes ” normal”.
In any case, let me here tackle the basics in stroke prevention. Just straight talk, the kind you may not hear from many of your doctors.
1) IF YOU ARE A SMOKER THEN QUIT SMOKING. That is probably the single best thing you can do yourself to cut down your risk of a stroke as well as a heart attack. There is no excuse, like I have cut down from a pack a day to about 3 cigarettes a day. NO AMOUNT OF SMOKING IS HEALTHY. You should quit completely if you want to cut down your risks of a heart attack or a brain attack (stroke). Now I do understand it is difficult to quit but here I am talking straight and not beating around the bush.
2) Exercise: again a thing which you can do yourself to reduce your risks of a heart attack or a stroke. The exercise which is recommended is more the aerobics kind. The idea is to increase your heart rate and sustain it at this level for some time. Running or brisk walking all are beneficial. Now before you do embark on a exercise program, run it past your doctor to make sure that you are fit enough to exercise. You do not want to strain a weak heart and exercise ideally should be graded. YOU START SLOW AND BUILD UP AS YOUR BODY GETS USED TO IT.
3) Blood pressure: we have known for a while now that elevated blood pressure is one of the most important risk factors for strokes. Recent studies have shown that the lower down you can get the blood pressure to, the more are the benefits. Earlier we used to advise our patients to aim for 130/80 mm Hg, now we say go for 120/70 mm Hg especially if you have other risk factors like stroke or previous history of coronary artery disease. There are many different medications that can be used to bring down the elevated blood pressure but some are recommended more because they have other added benefits apart from just lowering the blood pressure. Prominent among these is a group of medications called the ACE inhibitors. My advise to you shall be to get your blood pressure checked and than have your doctor decide which blood pressure medication shall be the best for you.
5) Bad cholesterol: bad cholesterol may run in your family that is it might be genetic in etiology. So not all bad cholesterol is your fault and due to the fact that your diet is bad. In either case it is one of the major risk factors for strokes and heart attacks. When we measure the cholesterol in the blood ideally we should measure it in a fasting state (so the blood sample should be taken when you are fasting like in the morning before breakfast). We measure the total cholesterol level in the blood and then measure the differrnt fractions of cholesterol. Some as you know is what is called good cholesterol, this is called HDL or high density cholesterol. The other is bad cholesterol, the one which we want to be lower ideally. These include LDL or low density lipoprotein, triglycerides or TG and very low density lipoprotein (VLDL) among others. The goal is to raise the good cholesterol or HDL and lower the bad cholesterol like TG and LDL.
We aim for total cholesterol less than 200, LDL less than 100 (nowdays we are even more aggressive and may aim for it to be less than 70) and TG less than 200 too. These goals can be achieved by a combination of dietary modification, exercise and medications. Fish is rich in omega 3 fatty acids and raises your HDL or good cholesterol. So replace the red meat with more fish. There are a number of medications out there. The most commonly used class is called statins and they help to raise your HDL and lower your LDL by a few points. However if your TGs are elevated, you may need a different class of drug.
My advise get your lipid profile done in a fasting state, then discuss the results with your doctor and have him help you decide whether you need just dietary modification or drugs too.
6) Control your blood sugar: if you are a diabetic this is very important because diabetes too is a risk factor for stroke. My advise get your blood sugar checked frequently both in the fasting and post prandial (after eating) state. The goal is fasting blood sugar less than 107 and post prandial less than 200 (in the case of post prandial it depends upon the time after eating when the sugar is measured). Your doctor may also check your Hemoglobin A1 C, the ideal goal for this is less than 7. Recent study in New England Journal of Medicine suggested that too aggressive lowering of hemoglobin A1C causes more harm than good (if you lower it less than 6) and may infact increase mortality. Hence again speak to your doctor and determine your goals.
7) Reduce your stress: mental stress is a killer and nothing is more important than your health. Do meditation and whatever else that works for you.
8) Drink alcohol in moderation: old saying too much of anything is bad and that includes the spirits!!!
REMEMBER A STROKE PREVENTED IS A BRAIN SAVED!!!
Nitin Sethi, MD
I thought in this post I shall discuss a little about stroke rehabilitation. A stroke can be devastating and causes significant morbidity and mortality. Stroke survivors are frequently left behind with neurological deficits. Common deficits include: motor (weakness on one side of the body usually arm and leg), speech deficits (patients may be left with a significant disorder of language. We call this aphasia and patients may have either difficully in comprehending speech or in the fluency of speech. Their speech may be slow and halting. At times they also have what we refer to as nominal aphasia also called anomia. These patients experience difficulty in naming things, like for example if you show them a pen, they would not be able to tell you that it is a pen. They shall know what it is used for but cannot get the name out). Patients may be left behind with residual numbness on one side of the body and depending upon the location of the stroke they may experience difficulty with seeing one half of their visual field (we call this a field cut). Some stroke patients are disabled by ataxia or unsteady gait, others may have disabling cerebellar symptoms.
Stroke rehabilitation plays a big role in the care of stroke patients. Contrary to popular held views, rehabilitation starts right at the onset of stroke and not once the acute stroke is over and the patient is been discharged. Now most of the big hospitals in the United States have acute stroke units. One of the biggest tenants of these acute stroke units is that rehabilitation is started soon after the patient presents to the hospital with an acute stroke. Studies have shown that the human brain has the maximum ability to heal and repair itself acutely (upto 6 months to a year) after a stroke. As time goes on, the brain loses this plasticity and the neurological deficits become more or less fixed. Thus rehabilitation in the acute stroke setting plays a vital role. Usually patients are evaluated by physical medicine doctors (rehab doctors) while they are still in the hospital with the acute stroke. An assessment is made of their deficits and depending upon that we decide which rehabilitation services are needed. Patients may get physical and occupational therapy in the hospital. They may also be seen by a speech and language therapist so that speech therapy can begin.
Nowdays there are many different modalities of rehablitation therapy which have been proven to be of benefit to patients with stroke. One of the popular ones is constraint induced movement therapy. In this the good arm of the patient is immobilized so that the patient is forced to use the weak arm. Melodic intonation therapy has recently gained popularity too. This therapy uses a style of singing called melodic intonation to stimulate activity in the right hemisphere of the brain in order to assist in speech production in patients who have aphasia.
Stroke rehabilitation does not end once the patient is discharged from the hospital. Most of these patients benefit from ongoing rehab (as I stated earlier this mostly occurs in the first 6-12 months). Patients may either be discharged to a rehab unit or a sub acute rehabilitation facility where these therapies can be carried out in a less hospital like atmosphere.
It is Saturday afternoon New York time. I though pen this from across the seven seas (I am on vacation!!). Hope some of you find this useful.
Personal Regards,
Nitin Sethi, MD
A comprehensive review on mind-body interventions and its application in various neurological disorders was recently published in Neurology. The authors Wahbeh, Elas and Oken searched Medline and PsychoInfo databases to identify clinical trials, reviews and published evidence on mind-body therapies and neurological diseases.
Meditation, relaxation, breathing exercises, yoga, tai-chi, qigong, hypnosis and biofeedback are some of the mind-body interventions that have been used in various neurological conditions like general pain, back and neck pain, carpel tunnel syndrome, headaches (migraine and tension), fibromyalgia, multiple sclerosis, epilepsy, neuromuscular diseases, stroke, falls with aging, Parkinson disease, stroke and attention deficit hyperactivity disorder (ADHD).
The authors do a good job in shifting through all the data to try to identify the effectiveness of mind-body interventions. As they point out in their discussion , many patients as many as 62% use complementary and alternative medicine therapies (CAM). Some with and many without the knowledge of their physicians. One of the reason why CAM therapies are popular is that they are relatively easy to implement, cheap (though many patients have to pay out of their pocket. Some insurance companies shall reimburse if you have a letter from your doctor) and more importantly as the authors point out it makes the patients feel empowered. They feel that they are in control of some of the decision making in their disease process and treatment. Moreover it gives a sense of general well being.
The authors righly point out that is difficult to scientifically judge whether these interventions are all effective. The reason for this is that many of the studies included small number of subjects and some of them did not have a control group. Moreover it is hard to blind these studies so as to avoid a placebo effect. Like suppose I want to study whether acupuncture is effective for lower back pain. One group I give acupuncture. Ideally I should have a control, a group which receives sham acupuncture so as to null the placebo effect. Now this is difficult to implement.
Th authors in their review conclude that there are several neurological conditions where the evidence in favor of mind-body therapies is quite strong such as migraine headaches. In other conditions the evidence is limited due to small clincial trials and inadequate control group.
It is reasonable to conclude that CAM therapies like yoga, tai-chi and qigong improve balance in the elderly and decrease the incidence of falls. Moreover they give a sense of well being and happiness. Meditation exercises whether it is mindfulness meditation, transcendental meditation or concentration meditation with the repetition of a word like Om or a mantra
“Hare Krishna Hare Krishna
Krishna Krishna Hare Hare
Hare Rama Hare Rama
Rama Rama Hare Hare”
all help in relaxation and reducing stress. This may decrease blood pressure and reduce the incidence of strokes and heart attacks. Brain changes have been observes during meditation in EEG and imaging studies and there is evidence that these exercises have wide spread effects on the endocrine and immune systems as well neurotransmitters. Hatha yoga may help in improving mobility and balance and thus decreasing fall risk. As the authors point out righly Bikram yoga which is carried out in very hot temperatures is likely not good for patients with MS, as it may worsen their weakness. This is called Uhthoff phenomena.
There is also some evidence to suggest benefits of these interventions in patients who have chronic lower back and neck pain, those with fibromyalgia, osteoarthritis as well as carpel tunnel syndrome (some studies suggest benefit while others do not).
My advise to patients who want to try out CAM therapies for various neurological conditions is to take their doctors into confidence. It is likely that some of these therapies when used along with allopathic medicines shall give added benefits and likely make you feel better. Like with any other therapy one must find a knowledgeable practitioner who knows what he or she is doing.
Then one can truly reap the benefits of these ancient therapies.
Personal Regards,
Nitin Sethi, MD

You must be logged in to post a comment.