Should transgender athletes be allowed to participate in combat sports? Will this be a fair bout and more importantly a safe bout (from the perspective of health and safety of both the combatants)? Attached is a PowerPoint presentation where in I discuss this polarizing topic.
Author: braindiseases
I am a qualified neurologist with sub specialization in the fields of epilepsy, clinical neurophysiology, sleep medicine and traumatic brain injury.
Helping the helpers…preventing burnout in caregivers of patients with dementia
Burnout rates are high in caregivers of patients with dementia. India currently lacks services such as day care centers, specialized nursing homes or availability of home health aides to address the needs of dementia patients. In this blogpost we highlight this problem and offer some innovative solutions to address this issue. P K SETHI, MD & N K SETHI, MD
Image source: Alzheimer’s Association of North CA.
Me and my migraine headaches
Migraine is one of the most common neurological disorder which a neurologist encounters during his or her practice. It is not without reason that it is often referred to as the bread and butter of neurological specialty. My parents are both physicians. My father is a neurologist and mother a pediatrician. Growing up I remember my mother coming back from the hospital and complaining of a throbbing migraine. She would lie down in a quiet dark room and ask me or my sister to press her head. Sometimes she would ask me to tie a “dupatta” (a shawl-like scarf worn by Indian women) tightly around her head in a vice-like grip. She never threw up during a migraine attack, but I remember she was always drained afterwards. My sister is 4 years older than me and when she entered high school and later medical college she too complained of severe migraines.
Following my father’s footsteps, I chose neurology as my specialty. My first recollection of getting migraine headaches is when I was in medical school. During residency training it was not uncommon for me to have a throbbing unilateral headache after an overnight call. By 10 am I would sign-out to my co-resident and head home. I would feel sick and realized quickly that if I ate a good breakfast, took an over the counter non-steroidal anti-inflammatory drug and fell asleep, I would wake up later that afternoon migraine free. I am now in my mid 40’s. As an academic neurologist, I see a wide variety of neurology patients including those who suffer from migraines. I am now able to better appreciate and characterize my own headache disorder. I suffer from common migraines. My typical migraine attack has no preceding visual aura. Just like the textbook description my headache is throbbing, pulsatile with pain radiating to the ipsilateral eye. I am light sensitive though sounds do not bother me as much. Most of my migraine attacks are left temporal. My migraine attacks share some characteristics which have been reported in the scientific literature. Professor Lance famously described the Red Ear Syndrome in migraineurs. Just as he described it, my ipsilateral ear becomes red and burns when I get a migraine attack. Sometimes both my ears become red and the red ear precedes the headache. I do not suffer from the Red Forehead Dot syndrome, a syndrome which I described along with my father. I have noticed things which have not been described in the migraine literature such as that I tend to tolerate my left temporal migraines better than the rarer right temporal ones. When I do get right temporal headaches, I feel very uneasy and irritable. On those occasions you may find me a bit short-tempered. When my migraine does not abort and persists for a long period of time, I develop subtle signs of cerebral dysfunction. I subjectively feel that my speech is off and that I am slurring, my typing skills deteriorate, and I frequently hit the wrong key. Very rarely I feel my balance off.
Over the years I have identified my migraine triggers. Stress at work especially when I am pressed for time and miss a meal is my most common trigger. Others include lack of sleep, dehydration, and red wine. An unusual one is perfumes with strong fruity fragrance. Recently an article highlighted the link between smartphone use and primary headache. Smartphone use does not trigger my typical migraine attack but when I am having a migraine attack, I am quite sensitive to my iPhone screen and ringtone. Multitasking on the computer and iPhone apps such as answering multiple text messages, e-mails and phone calls all increase the severity of my migraine attack. Overtime I have learnt to adapt to these necessary technological evils. My office computer and iPhone screen brightness are set to low, ringtone to Chimes and the Night Shift turned on from 7:00 pm to 7:00 am. I have my office lights dimmed at all time. Doctors are said to make the worst patients. I am guilty as charged and have resisted a drug for migraine prophylaxis. Recently due to an increase in the frequency of migraine attacks, I started amitriptyline 10 mg at night. The results have been gratifying. My migraine frequency has dramatically decreased but I wake up feeling groggy. My illness has made me better appreciate the impact of this chronic common neurological disease.
Nitin K Sethi, MD, MBBS, FAAN
COVID-19 and combat sports: when and how to begin bouts again?
COVID-19 and combat sports: when and how to begin bouts again?
Nitin K Sethi, MD
Department of Neurology, New York-Presbyterian Hospital, Weill Cornell Medical Center, New York, NY (U.S.A.)
DISCLOSURES: NKS serves as Associate Editor, The Eastern Journal of Medicine and Editor-in-Chief, ARP Journal of Combat Sports Medicine. He also serves as Chief Medical Officer of the New York State Athletic Commission (NYSAC). The views expressed are his and do not necessarily reflect the views of the NYSAC.
Professional boxing and mixed martial arts (MMA) are popular sports with a worldwide fanbase. COVID-19 (coronavirus disease 2019) is the infectious respiratory disease caused by SARS-COV 2 virus (Severe Acute Respiratory Syndrome coronavirus 2). On March 11th,2020 The World Health Organization (WHO) declared COVID-19 a pandemic considering the over 118,000 cases of the coronavirus illness in over 110 countries and territories around the world and the sustained risk of further global spread. 1 In order to control the spread of COVID-19, heath care authorities in different countries recommended isolation of sick persons, quarantine for those who may been exposed to the virus and social distancing. 2 Social distancing also referred to as physical distancing meant keeping space between people outside of their homes. A distance of at least 6 feet (2 meters) was recommended and people were asked not to gather in large groups, avoid crowded places and mass gatherings. Widespread cancelation or postponement of sporting events including boxing and MMA bouts followed. The most common sited cause for cancelation was fear of contagion. The encyclopedia describes contagion as the communication of disease from one person to another by close contact. By canceling events, State Commissions, promoters and combat sport’s governing bodies made the tough but responsible decision to protect all the concerned parties namely the athletes, their camps, Commission officials, production crews and the fans at the venue.
The global death toll from COVID-19 has been devastating. COVID-19 has infected more than 2 million people and killed at least 132,276 worldwide as of April 15th 2020 according to the coronavirus resource center at Johns Hopkins University. 3 The pandemic affected each and every one of us fundamentally changing the way we live our lives. The pandemic has peaked in many European countries and the United States. While deaths continue to mount, new cases and admissions are declining. Governments are now turning to the complex question of how and when to open different states and countries to business and normal life. For combat sports to resume this summer we should explore the possibility of initially holding events “behind closed doors”. Only the athletes, cornermen, referee, judges, Commission officials, ringside physicians and TV production crew would be present at the venue. The rationale for holding an event behind closed doors will be to reduce the risk of COVID-19 transmission from person to person by restricting the number of people at the venue to under 50. In the past month many SARS-COV 2 diagnostic test kits have become available. Some of these can be administered at the point-of-care with a turnaround time of 24 hours. It is proposed that all (not just combatants) present at the closed door event undergo a coronavirus screening questionnaire and be tested for SARS-COV 2 in the week leading up to the event. Social distancing should be practiced at the time of the weigh-ins and also the event itself. Corner men, referee, judges, Commission officials, ringside physicians and TV production crew should wear a surgical face mask (N 95 respirator is not warranted), gloves and eye-protection during the course of the event.
We should acknowledge that even if an event is held behind closed doors and all those present (not just the athletes) are tested for the coronavirus, the risk of transmission from person to person remains. Controlling the spread of the COVID-19 pandemic is far bigger than any boxing or MMA event. It is a matter of social responsibility and an obligation to act for the benefit of the society at large. By adopting some of the above practices a cautious start to combat sports events can be contemplated.
COVID-19 and telemedicine: old barriers come down and new ones come up
COVID-19 and telemedicine: old barriers come down and new ones come up
Nitin K Sethi, MD
Department of Neurology, New York-Presbyterian Hospital, Weill Cornell Medical Center, New York, NY (U.S.A.)
In the space of a few weeks the COVID-19 pandemic has changed the way medicine is practiced in the United States. In order to control the spread of COVID-19, the Centers for Disease Control and Prevention (CDC) and department of health (DOH) of various states recommended isolation of sick persons, quarantine for those who may been exposed to the virus and social distancing. Social distancing also referred to as physical distancing meant keeping space between people outside of their homes. A distance of at least 6 feet (2 meters) was recommended and people were asked not to gather in large groups, avoid crowded places and mass gatherings. All non-essential staff were advised to stay home and work remotely if the facility to do so was available to them. Hospitals across the country were forced to make some drastic changes in order to prepare for the expected surge of COVID-19 patients. In New York City, hospitals canceled all elective surgeries, closed in-patient epilepsy and stroke units and canceled all outpatient clinics. Patients were discharged from the hospitals. Beds especially ICU beds and other resources such as ventilators were reserved for COVID-19 patients. Physicians working in these hospitals were advised to adopt telemedicine in order to primarily maintain continuity of care for their existing patients. Barriers which over years had started to shackle the physician-patient relationship and physician autonomy in the practice of medicine came tumbling down. The Health Insurance Portability and Accountability Act (HIPAA), a US law designed to provide privacy standards to protect patients’ medical records and other health information provided to health plans, doctors, hospitals and other health care providers was relaxed to state that covered health care providers will not be subject to penalties for violations of the HIPAA Privacy, Security, and Breach Notification Rules that occur in the good faith provision of telehealth during the COVID-19 nationwide public health emergency. While physicians were encouraged to practice telehealth through their existing electronic health record (EHR) software, other modalities for pursuing telehealth were approved. Telehealth could be pursed via Zoom, WhatsApp or FaceTime. For physicians and patients who are unable to use any of the above modalities, a telephone encounter could be carried out. The above measures are a welcome relief to both physicians and patients as it helps maintain continuity of essential medical care during the COVID-19 pandemic. But just as the old barriers seem to come down, new ones started to come up. The HHS Office of Civil Rights (OCR) recommended the following: “OCR expects health care providers will ordinarily conduct telehealth in private settings, such as a doctor in a clinic or office connecting to a patient who is at home or at another clinic. Providers should always use private locations and patients should not receive telehealth services in public or semi-public settings, absent patient consent or exigent circumstances. If telehealth cannot be provided in a private setting, covered health care providers should continue to implement reasonable HIPAA safeguards to limit incidental uses or disclosures of protected health information (PHI). Such reasonable precautions could include using lowered voices, not using speakerphone, or recommending that the patient move to a reasonable distance from others when discussing PHI.” Overnight it seems new documentation guidelines came out with respect to televisits. We were told that physician documentation should include time start/end, participants on call and physical location of the patient at the time of the televisit. There had to be documentation of verbal consent that the patient understood that this is a billable visit. Patient could not have a phone visit within 7 days following last evaluation and could not be scheduled for an in-patient visit within 24 hours after a telephone visit else the physician could not bill for the televisit. We were informed of new billing codes and Medicare and Commercial Insurance rates for different time duration visits (5-10 minutes, 11-20 minutes, >21 minutes). A flurry of e-mails from the compliance specialists, medical billing specialists and office managers followed informing us of what we could or could not do. It has been said that the COVID-19 pandemic is going to change the world as we knew it. When it comes to the practice of medicine the rules are expected to change too. While some old barriers have thankfully fallen, unfortunately new barriers have come up. It seems removing the shackles is easier said than done.
COVID-19 and combat sports-to fight or not to fight?
COVID-19 and combat sports: to fight or not to fight?
Nitin K Sethi, MD
Department of Neurology, New York-Presbyterian Hospital, Weill Cornell Medical Center, New York, NY (U.S.A.)
DISCLOSURES: NKS serves as Associate Editor, The Eastern Journal of Medicine and Editor-in-Chief, ARP Journal of Combat Sports Medicine. He also serves as Chief Medical Officer of the New York State Athletic Commission (NYSAC). The views expressed are his and do not necessarily reflect the views of the NYSAC.
Professional boxing and mixed martial arts (MMA) are popular sports with a worldwide fanbase. COVID-19 (coronavirus disease 2019) is the infectious respiratory disease caused by SARS-COV 2 virus (Severe Acute Respiratory Syndrome coronavirus 2). On March 11th,2020 The World Health Organization (WHO) declared COVID-19 a pandemic considering the over 118,000 cases of the coronavirus illness in over 110 countries and territories around the world and the sustained risk of further global spread. In order to control the spread of COVID-19, heath care authorities in different countries recommended isolation of sick persons, quarantine for those who may been exposed to the virus and social distancing. Social distancing also referred to as physical distancing meant keeping space between people outside of their homes. A distance of at least 6 feet (2 meters) was recommended and people were asked not to gather in large groups, avoid crowded places and mass gatherings. Widespread cancelation or postponement of sporting events including boxing and MMA bouts followed. The most common sited cause for cancelation was fear of contagion. The encyclopedia describes contagion as the communication of disease from one person to another by close contact. By canceling events, State Commissions, promoters and combat sport’s governing bodies made the tough but responsible decision to protect all the concerned parties namely the athletes, their camps, Commission officials, production crews and the fans at the venue.
Some promoters have explored the possibility of holding a combat sports event “behind closed doors”. Only the athletes, cornermen, referee, judges, Commission officials, ringside physicians and TV production crew would be present at the venue. The rationale for holding an event behind closed doors is to reduce the risk of COVID-19 transmission from person to person at the venue. It was further proposed that all athletes be tested for SARS-COV2 before entering the ring or cage. The term “behind closed doors” is used primarily in association with football (soccer) to describe matches played where spectators are not allowed in the stadium to watch. Soccer matches are played behind closed doors to punish a team when its fans display rowdy behavior and clash with the rival team supporters and is included in the FIFA Disciplinary Code. 3
Amid the COVID-19 pandemic should combat sports events be held behind closed doors? Crowd less bouts are rarely heard of in combat sports. Passionate frequently blood hungry fans vociferously and voraciously support their prizefighter and are as much a part of the sport as the athletes themselves. Combat sports athletes fight not just for fame and money, they fight for their fans in the venue. Holding a crowd less event takes the very essence and vibe out of a combat sports event. Just like water is the elixir of life, so is the combat sports fan to the sport itself. Even if an event is held behind closed doors and all those present (not just the athletes) are tested for the coronavirus, the risk of transmission from person to person remains. Controlling the spread of the COVID-19 pandemic is far bigger than any boxing or MMA event. It is a matter of social responsibility and an obligation to act for the benefit of the society at large.
The stunned brain: neuroanatomical correlates of an acute concussion in boxing
The stunned brain: neuroanatomical correlates of an acute concussion in boxing
 Nitin K Sethi, MD
Nitin K Sethi, MD
Department of Neurology, New York-Presbyterian Hospital, Weill Cornell Medical Center, New York, NY (U.S.A.)
Abstract
A concussion can be defined as a transient alteration of mental status due to biomechanical forces affecting the brain. Concussions are common in contact sports like boxing and mixed martial arts (MMA). In boxing frequently the goal is to win by causing a knockout (KO)/concussion though a fight may also be won by a body shot if the boxer is unable to continue. This is then ruled a technical knockout (TKO). In the case report that follows, the clinical semiology of an acute concussion in boxing is described and a speculative hypothesis about the neuroanatomical correlate of the syndrome is postulated.
Case Report
A-32-year old right handed professional male boxer with a record of 20 wins, no losses with 10 of the wins coming by way of knockout suffered a brutal KO during a high profile televised bout. The boxer went down with the head striking and then bouncing off the ring canvas. Immediately on impact with the ring canvas the boxer exhibited decerebrate posturing followed by a 20 second convulsion characterized by stiffening of the arms and low amplitude clonic jerks of the legs. The referee immediately signaled an end to the fight and motioned the ringside physician to enter the ring to tend to the downed fighter. Examination inside the ring revealed a conscious boxer (eyes open) with unresponsiveness (no response to commands). This conscious unresponsiveness state lasted for about one minute. Pupils were midsize, equal in size with sluggish response to light. The emergency medical service (EMS) personnel stationed ringside were summoned into the ring by the ringside physician. While maintaining spinal fixation, the boxer was placed in a hard cervical collar and lifted on to and strapped on a hard backboard. As this was been accomplished, the boxer suddenly became responsive and started punching the air with his gloved hands as if he was back in the midst of the bout. He was combative and attempting to get up from the board. He was restrained by the medical staff. After about 1 minute, he calmed down and became fully alert and oriented. He realized that the fight had been stopped because of a KO and requested the medical staff to allow him to get up. At the post-fight medical evaluation he was determined to have suffered an acute concussion and administered a 90 day medical suspension. A neurology clearance was also requested prior to return to competitive boxing.
Discussion
The 5th international conference on concussion in sport held in Berlin, October 2016 defined a sport related concussion (SRC) as a traumatic brain injury induced by biomechanical forces resulting in the rapid onset of short-lived impairment of neurological function that resolves spontaneously 1. However, in some cases, signs and symptoms may evolve over a number of minutes to hours. While SRC may result in neuropathological changes, the acute clinical signs and symptoms largely reflect a functional brain disturbance rather than a structural injury with no abnormality seen on standard structural neuroimaging studies such as CT or MRI.
The centripetal theory of cerebral concussion postulates that in a concussion there is a centripetal progression of strains from the outer surfaces to the core (midbrain and basal diencephalon) of the brain 2, 3, 4. The anatomical localization of memory is in the temporal lobes or orbitotemporal regions. As per the centripetal theory, less degree of force does not penetrate deep into the cortex and so while cognitive and memory dysfunction may result, consciousness is retained. Forces strong enough to penetrate through to the mesencephalic brainstem result in loss of consciousness. It is important to remember that the above theory and biomechanical concepts are largely based on primate research and not on humans. The observation that brainstem signs can occur in the absence of significant “cortical” symptomatology and that cortical signs can occur in the absence of significant “brainstem” symptomatology means that the centripetal theory explains some but not all of the varied clinical semiology of concussion. It is generally accepted that traumatic decerebration, short duration traumatic coma (loss of consciousness) and impact seizure are brainstem release phenomena in which cortical inhibition of normally suppressed brainstem activity is lost due to diffuse cerebral injury. It may also be that the above phenomena are primarily due to failure of activity in the mesencephalic reticular formation and with loss of brainstem reflex response without widespread cortical involvement. The amnestic symptoms noted during a concussion have been postulated to be due to a transient interruption or disturbance in the ascending cortical projections at the level of the mesencephalon. It is hence intriguing to think of a “brainstem concussion” distinct from a “cortical concussion” each with different clinical semiology and symptom complex 4.
The above described clinical semiology of an acute concussion in boxing has not been described thus far in the medical literature. While this “stunned brain syndrome” is unnerving to witness as a physician neurologist because of its dramatic presentation and rapid evolution; the syndrome is self-limited with the boxer returning to baseline neurological function usually in the ring itself. It likely has the bulk of its anatomical focus in the brainstem with some cortical and subcortical contribution.
Understanding the neuroanatomical correlates of an acute SRC as in boxing has important implications for our conceptual understanding of concussion and acute management of these injuries in the ring.
References
- McCrory P, Meeuwisse W, Dvorak J, et al Consensus statement on concussion in sport—the 5thinternational conference on concussion in sport held in Berlin, October 2016. British Journal of Sports Medicine 2017; 51:838-847.
- Ommaya A. Head injury mechanisms and the concept of preventative management: a review and critical synthesis. J Neurotrauma1995; 12:527–46.
- Ommaya AK, Gennarelli TA. Cerebral concussion and traumatic unconsciousness. Correlation of experimental and clinical observations of blunt head injuries. Brain1974; 97:633–54.
- McCrory P. The nature of concussion: a speculative hypothesis. British Journal of Sports Medicine 2001; 35:146-147.
Ensuring and Maintaining Brain Health of the Combat Sports Athlete
Ensuring and maintaining brain health of the combat sport athlete
Nitin K Sethi, MD
Department of Neurology, New York-Presbyterian Hospital, Weill Cornell Medical Center, New York, NY (U.S.A.)
DISCLOSURES: NKS serves as Associate Editor, The Eastern Journal of Medicine and Editor-in-Chief, ARP Journal of Combat Sports Medicine. He also serves as Chief Medical Officer of the New York State Athletic Commission (NYSAC). The views expressed are his and do not necessarily reflect the views of the NYSAC.
Combat sports such as professional boxing and mixed martial arts (MMA) are popular sports with high risk for both acute and chronic traumatic brain injuries (TBI). Unfortunately, combatants have died in the ring or soon after the completion of a bout usually due to an acute catastrophic neurological event such as an acute subdural hematoma (SDH); which has been documented to be the most common cause of boxing related mortality. Acute TBI is just the tip of the iceberg when it comes to neurological injuries caused by combat sports. Hidden under the surface and away from the eyes of the public and media are the equally devastating chronic neurological sequelae of boxing and MMA including but not limited to chronic posttraumatic headache, chronic posttraumatic dizziness, posttraumatic cognitive impairment, posttraumatic Parkinsonism, posttraumatic dementia, dementia pugilistica, punch drunk syndrome, chronic traumatic encephalopathy (CTE) and neuropsychological sequelae such as mood, behavioral changes and depression.
At present there are no validated imaging or bio fluid (blood, cerebrospinal fluid) biomarkers for concussion and many of the above chronic neurological sequelae of boxing and MMA. In the absence of biomarkers; prognostication of the brain health of a combat sports athlete is inherently difficult. Most combatants undergo neuroimaging at the time of applying for initial licensure to compete in combat sports. This entails a magnetic resonance (MRI) scan of the brain without contrast usually carried out on a 1.5 or 3 Tesla strength magnet. In some countries and Commissions in the United States, a computed tomography (CT) scan of the head is acceptable in lieu of the MRI brain. While neuroimaging prior to licensure helps detect incidental clinically silent structural lesions with a high risk of bleeding such as aneurysm, arteriovenous malformation, large cavernoma, vein of Galen malformation and brain tumors, it does not yield any useful information about the function of the brain. Hence combining structural imaging with a functional study of the brain such as a formal neurocognitive evaluation should be considered at the time of initial licensure. Neurocognitive testing is a way to measure brain function non-invasively. It uses paper-and-pencil tests or computerized tests to assess important aspects of cognition such as attention, memory (immediate recall, short-term, long-term, auditory, visual), language, reaction time, perception and so on after factoring in the IQ and formal education of the examinee. A formal neurocognitive evaluation carried out by a qualified neuropsychologist is extremely helpful to formally assess the function of the brain as well as the mind and to grade/score it. The above test combo carried out at the time of the initial licensure serves as the baseline against which future test results are compared.
The average professional career of a combat sports athlete spans 10 years. During their active career most combatants fight on an average 2-6 times per year. It is recommended that a combat sports athlete undergo repeat MRI brain and neurocognitive evaluation after every 3 years. If the MRI shows evidence of prior TBI such as an area of encephalomalacia or gliosis, diffuse axonal injury, micro hemorrhages and the neurocognitive scores show a demonstrable decline, the combatant should be flagged. These combatants may need further tests such as PET scan of the brain, an electroencephalogram (EEG) and referral to a neurologist. On a case by case some may be allowed to proceed with their career under close observation while others may be counseled to hang up their gloves in order to prevent further and at times irreversible brain damage.
The brain is like a muscle and needs to be exercised, nourished and nurtured. The more it is exercised the stronger it becomes. Use it or lose it has scientific validity. Combat sports athletes should be counseled about brain health and how to build their cognitive reserve by doing exercises such as crossword puzzles, playing chess, reading, writing, listening to music or learning a new language or musical instrument. Supplements such as magnesium oxide and vitamin B12 are generally acknowledged to be brain healthy. A brain healthy Mediterranean diet which entails cooking food in extra virgin olive oil, less of dairy, less of red meat, more fish, more nuts should be promoted.
It is further recommended that the various sports commissions in the United States and abroad and combat sport’s governing bodies coordinate to assist with the setting up of an online central neuroimaging and neurocognitive database so that neuroimaging and neurocognitive data can be shared in the different countries where the combatant may compete.
The above interventions shall help to maintain the brain health of the combat sports athlete.
Reference
1. Sethi NK. Neuroimaging in contact sports: Determining brain fitness before and after a bout. SA J. Sports Med. 2017. vol.29 n.1 http://dx.doi.org/10.17159/2078-516x/2017/v29i0a2390
Can we afford not to afford treatment of multiple sclerosis in India?
Can we afford not to afford treatment of multiple sclerosis in India?
Neha Pandita 1, MD, Anuradha Batra 1, MD, Prahlad K Sethi 1, MD, Nitin K Sethi 2, MD
1 Department of Neurology, Sir Ganga Ram Hospital, New Delhi (India)
2 Department of Neurology, New York-Presbyterian Hospital, Weill Cornell Medical Center, New York, NY (U.S.A.)
Multiple sclerosis (MS) is a chronic neurological disease which affects men and women in the prime of their youth. The disease can present in relapsing-remitting, secondary progressive, progressive relapsing and primary progressive forms and leads to increasing disability during the course of the patient’s lifespan. Symptoms such as muscle weakness, gait and balance problems, coordination problems, visual impairment, diplopia, bladder and bowel disturbances, sensory symptoms, cognitive dysfunction and fatigue can be disabling at times and lead to poor health related quality of life, neurological disability and high health care costs. Progressive disease can be paricularly disabling leading to a wheel chair chair dependent on caregivers for activities of daily living. In India; till a few years ago, MS was thought to be rare and a disease of the Western hemispher. It is unclear why now we are seeing more and more MS patients in India. Is it because with advances in health care and diagnostics, we are diagnosing more cases which earlier remained undiagnosed or is the incidece of this disease actually increasing in the Indian population? This still needs to be determined and it would behoove us well to start a national MS registry and keep a track of MS cases and coregister with dietary and enviromental variables. Many low and middle income countres such as India have a huge population with limited accessibility and affordability to health care facilities. About 70% of India’s 1.3 billion population lives in rural areas with 30% living below the poverty line. In a country like India, a disease like MS can have a particularly devastating impact not just because of its chronicity and propensity to affect the young but also due to its high treatment cost burden. A study published in April, 2015 found that the cost of first generation disease modifying medications for MS increased from between $8000 to $11000 annually in the 1990s to approximately between $60000 to S90000 per year currently. Newer disease modifying MS drugs cost even more.In the west, patients with MS commonly pay for their MS treatment in one of the following ways:
1. Job (employer) based health insurance plan
2. Individual health insurance plan
3. Medicare
4. Medicaid or state children’s health insurance program
5. Other state and federal government funded programs for the uninsured and underinsured
In India, where illiteracy, unemployment and poverty remain major social problems, state and federal supported health insurance schemes benefit only a small fraction of the population. As in India at present there is no National Health Insurance program, patients have to pay out of pocket for health care. The purpose of writing this commentary is to draw attention to the cost burden associated with a chronic disease like MS and start a discussion on treatment solutions that may benefit our MS population without causing unbearable financial burden.
We calculated the average health care cost to a patient who is first time admitted for any demyelinating disease, in a corporate health care institution. A patient with spastic paraparesis was admitted to Sir Ganga Ram Hospital (SGRH) with provisional diagnosis of acute myelitis later confirmed as MS. We found that the entire hospitalization cost him around Rs. 1.8 lac ($2560).
Breakdown of costs:
Investigations:
–contrast enhanced MRI brain and cervical spine (Rs. 26000/ $ 416)
–visual evoked potential (VEP) (Rs. 2000/$ 32 )
–lumbar puncture (CSF analysis) (Rs. 8000/ $ 128)
–ancillary investigations like autoimmune encephalitis panel (Rs. 40000/ $ 464).
Treatment costs:
—pulse IV steroid therapy x 5 days (Rs. 70000/ $ 1120)
Hospital stay costs:
–room cost plus ancillary expenditure (Rs. 70000/ $ 1120)
It is important to remember that this is the financial burden borne out of pocket by an average middle class patient admitted to SGRH. Patients who live below the poverty line cannot afford such costs and the financial burden forces family members to take loans or at times sell their home and property to pay for the treatment. Unlike a case of post infectious myelitis, a patient with MS may suffer an acute exacerabation or relapse leading to another hospitalization and additional costs. The various MS disease modifying agents are so expensive that few patients in India can afford the drugs. Many as a result discontinue treatment regimens and self medicate with medications such as oral steroids.
We also calculated the average cost to the patient of various disease modifying agents available in India.
1. Injectable DMTs like Avonex (beta interferon) given at a dose of 30mcg I/M once a week costs Rs. 30000/ $ 480 dollars monthly.
2. Copaxone (glatiramer acetate) Rs. 20000/ $ 320 monthly.
3. Mitoxantrone Rs. 400/ $ 5 per vial
4. Tysabri (natalizumab) costs a whopping Rs. 1,40,800/ S 2184 monthly.
5. Oral DMTs like fingolimod costs around Rs. 3,00,000/ S 4790 dollar for 30 capsules, teriflunomide Rs. 2,90,000/ $ 4500 for 1 month supply, and dimethyl fumarate Rs. 3,40,000/ $ 5300 for 1 month supply.
6. Azathioprine costs Rs. 600/ $ 9.6 per month
The per capita income in India is estimated at just short of Rs. 6000 per month which equals $ 90 per month. That means the per capita income for a family of 4 would be less than $ 400 a month, but the reality is that most people live on much less than that and struggle to provide for the basic needs of food, clothing and shelter. Both the interferons and the oral DMTs are accessible to only a few in India due to their exorbant cost. As a result, many Indian MS patients cannot afford treatment and are left behind untreated with significant neurological disability impairing their quality of life. In India, where it is estimated that around 100,000-200,000 people have MS, finding cost effective treatment options is very important.
What are the solutions?
1. Methylprednisolone (Solumedrol) is an effective drug used to treat an acute attack of MS. Once the diagnosis of MS is confirmed, and patient presents to the hospital with an acute exacerbation, first dose of methylprednisolone can be administered in the emergency department followed by rest of the doses at home. The outpatient administration can be carried out by trained nurses via patient outreach programs. This will greatly reduce the cost of treating an acute attack of MS without requiring admission.
2. An initial MS diagnostic and treatment package should be constituted, including all the necessary initial investigations and treatment. This shall help drive down the initial costs incurred by patients and family members.
3. A MRI package should be constituted. This should include the cost of MRI brain and cervical spine imaging at least once a year and help in reducing the diagnostic cost associated with repeated neuroimaging in patients with MS.
4. A National Health Insurance scheme geared towards chronic neurological diseases such as MS should be formulated. While many good insurance schemes have been recently launched by the government, unfortunately they remain on paper only.
5. Pharmaceutical companies manufacturing and marketing MS drugs should be approached by the government and the cost of MS drugs should be negotiated so that more patients can afford these medications and avail their benefits. Recently 3 Indian pharaceutical companies have launched generic versions of Tecfidera (dimethyl fumarate) costing under Rs.4000/month. Intas pharmaceuticals generic version of Aubagio (teriflunomide) costs only Rs. 2000/month.
6. There are various studies documenting the effectiveness of azathioprine in MS patients. A multicentre randomized non inferiority trial was conducted comparing azathioprine vs beta interferons for relapsing remitting multiple sclerosis and it was found that efficacy of azathioprine is not inferior to that of beta interferon for patients with relapsing remitting multiple sclerosis 1. Massacesi et al conducted a study evaluating the efficacy of azathioprine therapy on new brain lesions evaluated using magnetic resonance imaging and concluded that azathioprine administered at lymphocyte suppressing doses, is effective in reducing MS new brain inflammatory lesions and is well tolerated 2. In a study by Casetta et al in 698 patients with MS, it was concluded that azathioprine is a fair alternative to interferon beta for treating MS patients 3. In SGRH, we have around 20 patients with MS who are on azathioprine for the past 10 years, doing well and tolerating the medication well. Considering the convenience of oral administration, low cost and good efficacy, azathioprine may represent an alternative to interferon and oral DMTs. This should be studied further in the Indian context.
Conclusions
In India, there is a large unmet disease burden of MS. We can’t afford not to afford the treatment of MS in India as it affects our young population who are the backbone of our nation. To tailor to the requirements of the Indian population, drug trials with large sample size using cheaper drugs such as azotioprine are needed. Large academic medical centers in India should take the lead in this initiative and run head to head trials of azothioprine against more established injectables and oral DMTs.
Disseminated cysticercosis (tapeworm)in a vegetarian male
Disseminated cysticercosis (tapeworm) in a vegetarian male
Prahlad K Sethi, MD and Nitin K Sethi, MD,

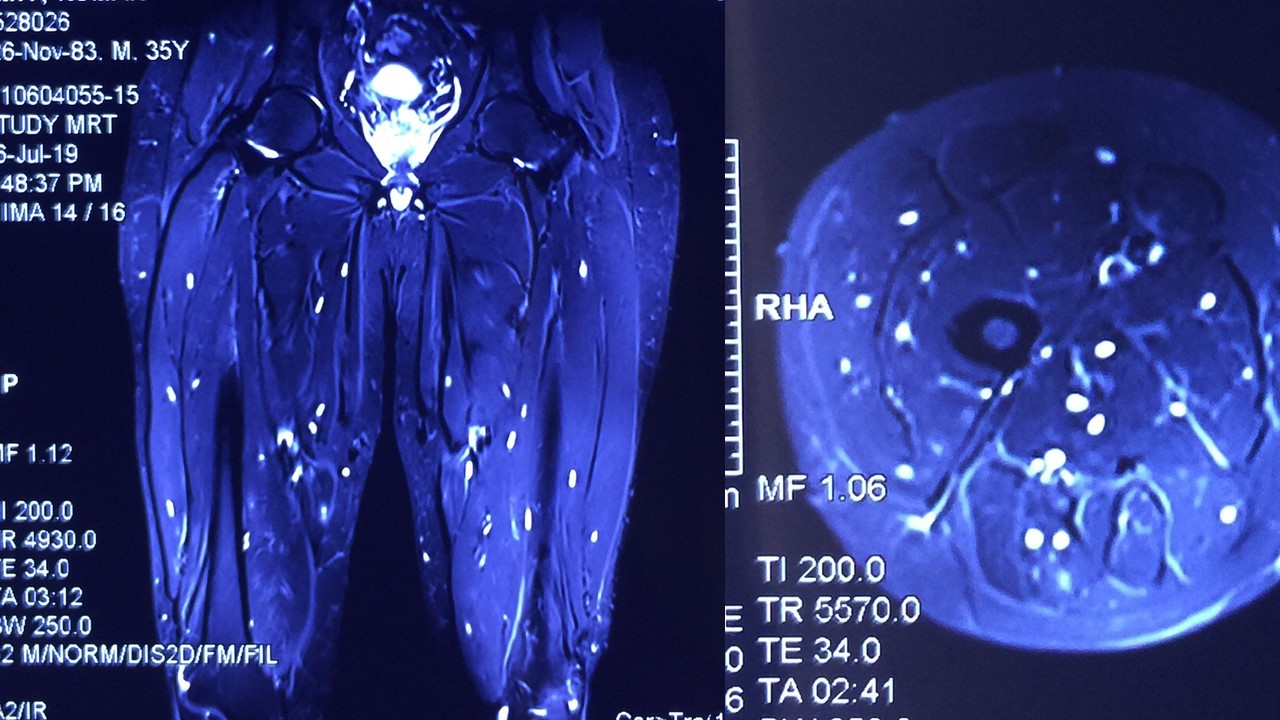
A 35-year-old vegetarian man presented with a generalized convulsion. MRI brain showed extensive cysticerci lesions involving the bilateral supra and infra-tentorial brain parenchyma, myofascial planes of the face, neck, floor of mouth, parotid glands and left orbital extraocular muscles (figure 1). MRI thigh showed diffuse cysticerci involving multiple muscles (figure 2). Disseminated cysticercosis can occur in vegetarians and non-pork eaters due to fecal-oral contamination of food with Taenia solium eggs from tapeworm carriers1.

You must be logged in to post a comment.