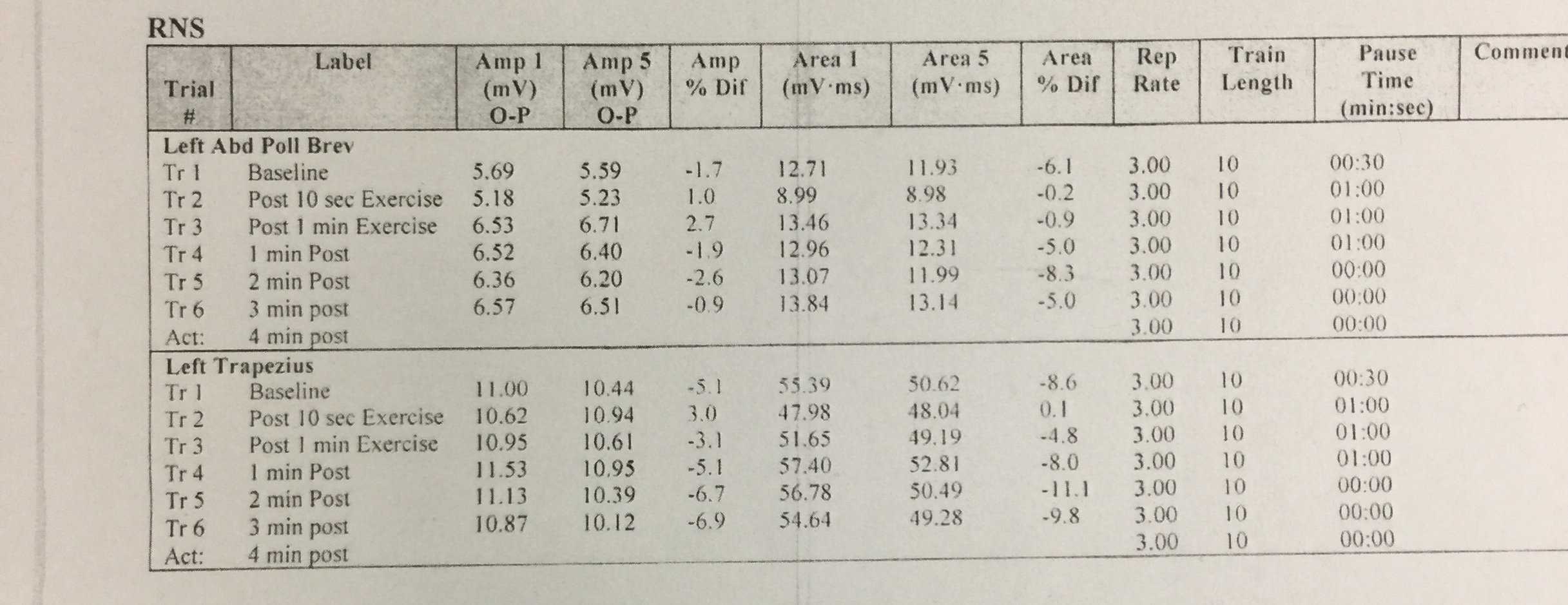
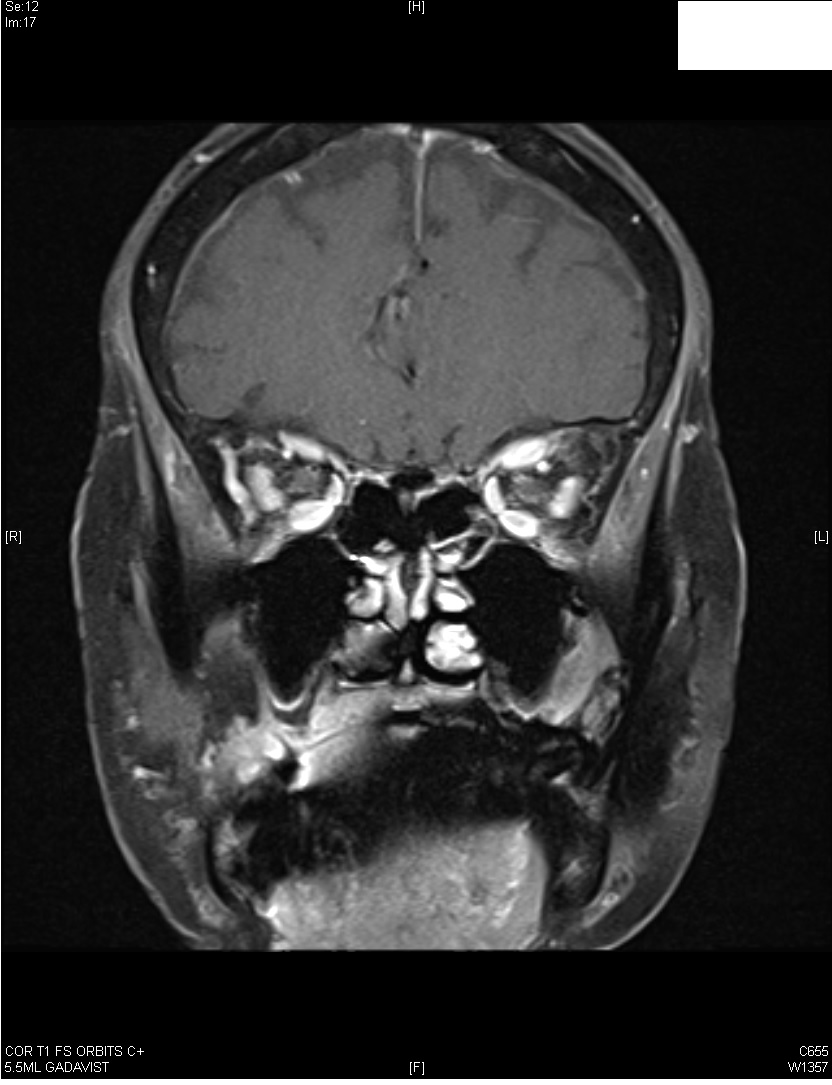
A 84-year-old right handed lady presented with 2 months history of diplopia on binocular vision worse on right gaze. On monocular vision, diplopia disappeared irrespective of which eye was closed. AchR binding Ab was 1.07 nmol/L (positive >0.5 nmol/L) and she was diagnosed with myasthenia gravis. Neurological examination was normal. Nerve conduction studies and needle EMG of all muscles was within normal limits. Repetitive nerve stimulation at 3 Hz of the left medial nerve/APB and accessory nerve/trapezius system, at rest and following 10 seconds and 60 seconds of exercise revealed no abnormal decremental or incremental response (figure 1). MRI brain revealed enlargement and abnormal enhancement of the muscle bellies of the bilateral superior, medial and inferior rectus muscles in pattern suggestive of thyroid orbitopathy (figure 2).TSH 3rd generation was 0.145 (range 0.550-4.780 uIU/mL. Thyroid associated orbitopathy, also known as Graves’ orbitopathy, is typically a self-limiting autoimmune process associated with dysthyroid states with clinical presentation varying from mild disease to severe irreversible sight-threatening complications. 1
Reference
1. Maheshwari R, Weis E. Thyroid associated orbitopathy. Indian J Ophthalmol. 2012; 60: 87–93.